World
Topics from outside of this forum. Views and opinions represented here may not reflect those of this forum and its members.
-
This is a community for medical professionals. Please see the Medical Community Hub for other communities.
Official Lemmy community for /r/Medicine.
!medicine@mander.xyz is a virtual lounge for physicians and other medical professionals from around the world to talk about the latest advances, controversies, ask questions of each other, have a laugh, or share a difficult moment.
This is a highly moderated community. Please read the rules carefully before posting or commenting.
Related Communities
- Medical Community Hub
- Medicine (📍)
- Medicine Canada
- Premed
- Premed Canada
- Public Health
See the pinned post in the Medical Community Hub for links and descriptions. link (!medicine@lemmy.world)
Rules
Violations may result in a warning, removal, or ban based on moderator discretion. The rule numbers will correspond to those on /r/Medicine, and where differences are listed where relevant. Please also remember that instance rules for mander.xyz will also apply.
-
Flairs & Starter Comment: Lemmy does not have user flairs, but you are welcome to highlight your role in the healthcare system, however you feel is appropriate. Please also include a starter comment to explain why the link is of interest to the community and to start the conversation. Link posts without starter comments may be temporarily or permanently removed. (rule is different from /r/Medicine)
-
No requests for professional advice or general medical information: You may not solicit medical advice or share personal health anecdotes about yourself, family, acquaintances, or celebrities, seek comments on care provided by other clinicians, discuss billing disputes, or otherwise seek a professional opinion from members of the community. General queries about medical conditions, prognosis, drugs, or other medical topics from the lay public are not allowed.
-
No promotions, advertisements, surveys, or petitions: Surveys (formal or informal) and polls are not allowed on this community. You may not use the community to promote your website, channel, community, or product. Market research is not allowed. Petitions are not allowed. Advertising or spam may result in a permanent ban. Prior permission is required before posting educational material you were involved in making.
-
Link to high-quality, original research whenever possible: Posts which rely on or reference scientific data (e.g. an announcement about a medical breakthrough) should link to the original research in peer-reviewed medical journals or respectable news sources as judged by the moderators. Avoid login or paywall requirements when possible. Please submit direct links to PDFs as text/self posts with the link in the text. Sensationalized titles, misrepresentation of results, or promotion of blatantly bad science may lead to removal.
-
Act professionally and decently: /c/medicine is a public forum that represents the medical community and comments should reflect this. Please keep disagreement civil and focused on issues. Trolling, abuse, and insults (either personal or aimed at a specific group) are not allowed. Do not attack other users’ flair. Keep offensive language to a minimum and do not use ethnic, sexual, or other slurs. Posts, comments, or private messages violating Reddit’s content policy will be removed and reported to site administration.
-
No personal agendas: Users who primarily post or comment on a single pet issue on this community (as judged by moderators) will be asked to broaden participation or leave. Comments from users who appear on this community only to discuss a specific political topic, medical condition, health care role, or similar single-topic issues will be removed. Comments which deviate from the topic of a thread to interject an unrelated personal opinion (e.g. politics) or steer the conversation to their pet issue will be removed.
-
Protect patient confidentiality: Posting protected health information may result in an immediate ban. Please anonymize cases and remove any patient-identifiable information. For health information arising from the United States, follow the HIPAA Privacy Rule’s De-Identification Standard.
-
No careers or homework questions: Questions relating to medical school admissions, courses or exams should be asked elsewhere. Links to medical training communitys and a compilation of careers and specialty threads are available on the /r/medicine wiki. Medical career advice may be asked. (rule is different from /r/Medicine)
-
Throwaway accounts: There are currently no limits on account age or ‘karma’. (rule is different from /r/Medicine)
-
No memes or low-effort posts: Memes, image links (including social media screenshots), images of text, or other low-effort posts or comments are not allowed. Videos require a text post or starter comment that summarizes the video and provides context.
-
No Covid misinformation, conspiracy theories, or other nonsense
Moderators may act with their judgement beyond the scope of these rules to maintain the quality of the community. If your post doesn’t show up shortly after posting, make sure that it meets our posting criteria. If it does, please message a moderator with a link to your post and explanation. You are free to message the moderation team for a second opinion on moderator actions.
-
Posts from the RSS Feed of HackerNews.
The feed sometimes contains ads and posts that have been removed by the mod team at HN.
-
my journal
-
A community to post scientific articles, news, and civil discussion.
rule #1: be kind
-
A Fediverse community for open-ended, thought provoking questions
Rules: (interactive)
1) Be nice and; have funDoxxing, trolling, sealioning, racism, and toxicity are not welcomed in AskLemmy. Remember what your mother said: if you can’t say something nice, don’t say anything at all. In addition, the site-wide Lemmy.world terms of service also apply here. Please familiarize yourself with them
2) All posts must end with a '?'This is sort of like Jeopardy. Please phrase all post titles in the form of a proper question ending with ?
3) No spamPlease do not flood the community with nonsense. Actual suspected spammers will be banned on site. No astroturfing.
4) NSFW is okay, within reasonJust remember to tag posts with either a content warning or a [NSFW] tag. Overtly sexual posts are not allowed, please direct them to either !asklemmyafterdark@lemmy.world or !asklemmynsfw@lemmynsfw.com. NSFW comments should be restricted to posts tagged [NSFW].
5) This is not a support community.It is not a place for ‘how do I?’, type questions. If you have any questions regarding the site itself or would like to report a community, please direct them to Lemmy.world Support or email info@lemmy.world. For other questions check our partnered communities list, or use the search function.
6) No US Politics.Please don’t post about current US Politics. If you need to do this, try !politicaldiscussion@lemmy.world or !askusa@discuss.online
Reminder: The terms of service apply here too.
Partnered Communities:
Logo design credit goes to: tubbadu
-
/c/TenForward: Your home-away-from-home for all things Star Trek!
Re-route power to the shields, emit a tachyon pulse through the deflector, and post all the nonsense you want. Within reason of course.
~ 1. No bigotry. This is a Star Trek community. Remember that diversity and coexistence are Star Trek values. Any post/comments that are racist, anti-LGBT, or generally “othering” of a group will result in removal/ban.
~ 2. Keep it civil. Disagreements will happen both on lore and preferences. That’s okay! Just don’t let it make you forget that the person you are talking to is also a person.
~ 3. Use spoiler tags. This applies to any episodes that have dropped within 3 months prior of your posting. After that it’s free game.
~ 4. Keep it Trek related. This one is kind of a gimme but keep as on topic as possible.
~ 5. Keep posts to a limit. We all love Star Trek stuff but 3-4 posts in an hour is plenty enough.
~ 6. Try to not repost. Mistakes happen, we get it! But try to not repost anything from within the past 1-2 months.
~ 7. No General AI Art. Posts of simple AI art do not ‘inspire jamaharon’
~ 8. No Political Upheaval. Political commentary is allowed, but please keep discussions civil. Read here for our community’s expectations.
Fun will now commence.
Sister Communities:
Want your community to be added to the sidebar? Just ask one of our mods!
Creator Resources:
Looking for a Star Trek screencap? (TrekCore)
Looking for the right Star Trek typeface/font for your meme? (Thank you @kellyaster for putting this together!)
-
A “Showerthought” is a simple term used to describe the thoughts that pop into your head while you’re doing everyday things like taking a shower, driving, or just daydreaming. The most popular seem to be lighthearted clever little truths, hidden in daily life.
Here are some examples to inspire your own showerthoughts:
- Both “200” and “160” are 2 minutes in microwave math
- When you’re a kid, you don’t realize you’re also watching your mom and dad grow up.
- More dreams have been destroyed by alarm clocks than anything else
Rules
- All posts must be showerthoughts
- The entire showerthought must be in the title
- No politics
- If your topic is in a grey area, please phrase it to emphasize the fascinating aspects, not the dramatic aspects. You can do this by avoiding overly politicized terms such as “capitalism” and “communism”. If you must make comparisons, you can say something is different without saying something is better/worse.
- A good place for politics is c/politicaldiscussion
- Posts must be original/unique
- Adhere to Lemmy’s Code of Conduct and the TOS
If you made it this far, showerthoughts is accepting new mods. This community is generally tame so its not a lot of work, but having a few more mods would help reports get addressed a little sooner.
Whats it like to be a mod? Reports just show up as messages in your Lemmy inbox, and if a different mod has already addressed the report, the message goes away and you never worry about it.
-
No such thing. Ask away!
!nostupidquestions is a community dedicated to being helpful and answering each others’ questions on various topics.
The rules for posting and commenting, besides the rules defined here for lemmy.world, are as follows:
Rules (interactive)
Rule 1- All posts must be legitimate questions. All post titles must include a question.All posts must be legitimate questions, and all post titles must include a question. Questions that are joke or trolling questions, memes, song lyrics as title, etc. are not allowed here. See Rule 6 for all exceptions. _____________
:::spoiler Rule 2- Your question subject cannot be illegal or NSFW material.
Your question subject cannot be illegal or NSFW material. You will be warned first, banned second.
:::
:::spoiler Rule 3- Do not seek mental, medical and professional help here.
Do not seek mental, medical and professional help here. Breaking this rule will not get you or your post removed, but it will put you at risk, and possibly in danger.
:::
:::spoiler Rule 4- No self promotion or upvote-farming of any kind.
That’s it.
:::
:::spoiler Rule 5- No baiting or sealioning or promoting an agenda.
Questions which, instead of being of an innocuous nature, are specifically intended (based on reports and in the opinion of our crack moderation team) to bait users into ideological wars on charged political topics will be removed and the authors warned - or banned - depending on severity.
:::
:::spoiler Rule 6- Regarding META posts and joke questions.
Provided it is about the community itself, you may post non-question posts using the [META] tag on your post title.
On fridays, you are allowed to post meme and troll questions, on the condition that it’s in text format only, and conforms with our other rules. These posts MUST include the [NSQ Friday] tag in their title.
If you post a serious question on friday and are looking only for legitimate answers, then please include the [Serious] tag on your post. Irrelevant replies will then be removed by moderators.
:::
:::spoiler Rule 7- You can’t intentionally annoy, mock, or harass other members.
If you intentionally annoy, mock, harass, or discriminate against any individual member, you will be removed.
Likewise, if you are a member, sympathiser or a resemblant of a movement that is known to largely hate, mock, discriminate against, and/or want to take lives of a group of people, and you were provably vocal about your hate, then you will be banned on sight.
:::
:::spoiler Rule 8- All comments should try to stay relevant to their parent content.
:::
:::spoiler Rule 9- Reposts from other platforms are not allowed.
Let everyone have their own content.
:::
:::spoiler Rule 10- Majority of bots aren’t allowed to participate here. This includes using AI responses and summaries.
:::
Credits
Our breathtaking icon was bestowed upon us by @Cevilia!
The greatest banner of all time: by @TheOneWithTheHair!
-
Community rules
1. Be civilNo trolling, bigotry or other insulting / annoying behaviour
2. No politicsThis is non-politics community. For political memes please go to !politicalmemes@lemmy.world
3. No recent repostsCheck for reposts when posting a meme, you can only repost after 1 month
4. No botsNo bots without the express approval of the mods or the admins
5. No Spam/Ads/AI SlopNo advertisements or spam. This is an instance rule and the only way to live. We also consider AI slop to be spam in this community and is subject to removal.
A collection of some classic Lemmy memes for your enjoyment
Sister communities
- !tenforward@lemmy.world : Star Trek memes, chat and shitposts
- !lemmyshitpost@lemmy.world : Lemmy Shitposts, anything and everything goes.
- !linuxmemes@lemmy.world : Linux themed memes
- !comicstrips@lemmy.world : for those who love comic stories.
-
A community for international relations; theory & news.
What is international relations?
- Keep discourse civil
-
Ask a science question, get a science answer.
Community Rules
Rule 1: Be respectful and inclusive.Treat others with respect, and maintain a positive atmosphere.
Rule 2: No harassment, hate speech, bigotry, or trolling.Avoid any form of harassment, hate speech, bigotry, or offensive behavior.
Rule 3: Engage in constructive discussions.Contribute to meaningful and constructive discussions that enhance scientific understanding.
Rule 4: No AI-generated answers.Strictly prohibit the use of AI-generated answers. Providing answers generated by AI systems is not allowed and may result in a ban.
Rule 5: Follow guidelines and moderators' instructions.Adhere to community guidelines and comply with instructions given by moderators.
Rule 6: Use appropriate language and tone.Communicate using suitable language and maintain a professional and respectful tone.
Rule 7: Report violations.Report any violations of the community rules to the moderators for appropriate action.
Rule 8: Foster a continuous learning environment.Encourage a continuous learning environment where members can share knowledge and engage in scientific discussions.
Rule 9: Source required for answers.Provide credible sources for answers. Failure to include a source may result in the removal of the answer to ensure information reliability.
By adhering to these rules, we create a welcoming and informative environment where science-related questions receive accurate and credible answers. Thank you for your cooperation in making the Ask Science community a valuable resource for scientific knowledge.
We retain the discretion to modify the rules as we deem necessary.
-
This is a most excellent place for technology news and articles.
Our Rules
- Follow the lemmy.world rules.
- Only tech related news or articles.
- Be excellent to each other!
- Mod approved content bots can post up to 10 articles per day.
- Threads asking for personal tech support may be deleted.
- Politics threads may be removed.
- No memes allowed as posts, OK to post as comments.
- Only approved bots from the list below, this includes using AI responses and summaries. To ask if your bot can be added please contact a mod.
- Check for duplicates before posting, duplicates may be removed
- Accounts 7 days and younger will have their posts automatically removed.
Approved Bots
-
Health: physical and mental, individual and public.
Discussions, issues, resources, news, everything.
See the pinned post for a long list of other communities dedicated to health or specific diagnoses. The list is continuously updated.
Nothing here shall be taken as medical or any other kind of professional advice.
Commercial advertising is considered spam and not allowed. If you’re not sure, contact mods to ask beforehand.
Linked videos without original description context by OP to initiate healthy, constructive discussions will be removed.
Regular rules of lemmy.world apply. Be civil.
-
Welcome to c/science_memes @ Mander.xyz!
A place for majestic STEMLORD peacocking, as well as memes about the realities of working in a lab.
Rules
- Don’t throw mud. Behave like an intellectual and remember the human.
- Keep it rooted (on topic).
- No spam.
- Infographics welcome, get schooled.
This is a science community. We use the Dawkins definition of meme.
Research Committee
Other Mander Communities
Science and Research
Biology and Life Sciences
- !abiogenesis@mander.xyz
- !animal-behavior@mander.xyz
- !anthropology@mander.xyz
- !arachnology@mander.xyz
- !balconygardening@slrpnk.net
- !biodiversity@mander.xyz
- !biology@mander.xyz
- !biophysics@mander.xyz
- !botany@mander.xyz
- !ecology@mander.xyz
- !entomology@mander.xyz
- !fermentation@mander.xyz
- !herpetology@mander.xyz
- !houseplants@mander.xyz
- !medicine@mander.xyz
- !microscopy@mander.xyz
- !mycology@mander.xyz
- !nudibranchs@mander.xyz
- !nutrition@mander.xyz
- !palaeoecology@mander.xyz
- !palaeontology@mander.xyz
- !photosynthesis@mander.xyz
- !plantid@mander.xyz
- !plants@mander.xyz
- !reptiles and amphibians@mander.xyz
Physical Sciences
- !astronomy@mander.xyz
- !chemistry@mander.xyz
- !earthscience@mander.xyz
- !geography@mander.xyz
- !geospatial@mander.xyz
- !nuclear@mander.xyz
- !physics@mander.xyz
- !quantum-computing@mander.xyz
- !spectroscopy@mander.xyz
Humanities and Social Sciences
Practical and Applied Sciences
- !exercise-and sports-science@mander.xyz
- !gardening@mander.xyz
- !self sufficiency@mander.xyz
- !soilscience@slrpnk.net
- !terrariums@mander.xyz
- !timelapse@mander.xyz
Memes
Miscellaneous
-
Just post something 💛
Lemmy’s general purpose discussion community with no specific topic.
Sitewide lemmy.world rules apply here.
Additionally, this is a no AI content community. We are here for human interaction, not AI slop! Posts or comments flagged as AI generated will be removed.
-
Welcome to the Unpopular Opinion community!
How voting works:
Vote the opposite of the norm.___ If you agree that the opinion is unpopular give it an arrow up. If it’s something that’s widely accepted, give it an arrow down. ___
Guidelines:
Tag your post, if possible (not required)___ * If your post is a “General” unpopular opinion, start the subject with [GENERAL]. * If it is a Lemmy-specific unpopular opinion, start it with [LEMMY]. ___
Rules:
1. NO POLITICS___ Politics is everywhere. Let’s make this about [general] and [lemmy] - specific topics, and keep politics out of it. ___
2. Be civil.___ Disagreements happen, but that doesn’t provide the right to personally attack others. No racism/sexism/bigotry. Please also refrain from gatekeeping others’ opinions.
3. No bots, spam or self-promotion.
______ Only approved bots, which follow the guidelines for bots set by the instance, are allowed. ___
4. Shitposts and memes are allowed but...___ Only until they prove to be a problem. They can and will be removed at moderator discretion. ___
5. No trolling.___ This shouldn’t need an explanation. If your post or comment is made just to get a rise with no real value, it will be removed. You do this too often, you will get a vacation to touch grass, away from this community for 1 or more days. Repeat offenses will result in a perma-ban. ___
6. Defend your opinion___ This is a bit of a mix of rules 4 and 5 to help foster higher quality posts. You are expected to defend your unpopular opinion in the post body. We don’t expect a whole manifesto (please, no manifestos), but you should at least provide some details as to why you hold the position you do. ___
Instance-wide rules always apply. legal.lemmy.world/tos/
-

Welcome to the largest gaming community on Lemmy! Discussion for all kinds of games. Video games, tabletop games, card games etc.
Rules
1. Submissions have to be related to gamesVideo games, tabletop, or otherwise. Posts not related to games will be deleted. This community is focused on games, of all kinds. Any news item or discussion should be related to gaming in some way.
2. No bigotry or harassment, be civilNo bigotry, hardline stance. Try not to get too heated when entering into a discussion or debate. We are here to talk and discuss about one of our passions, not fight or be exposed to hate. Posts or responses that are hateful will be deleted to keep the atmosphere good. If repeatedly violated, not only will the comment be deleted but a ban will be handed out as well. We judge each case individually.
3. No excessive self-promotionTry to keep it to 10% self-promotion / 90% other stuff in your post history. This is to prevent people from posting for the sole purpose of promoting their own website or social media account.
4. Stay on-topic; no memes, funny videos, giveaways, reposts, or low-effort postsThis community is mostly for discussion and news. Remember to search for the thing you’re submitting before posting to see if it’s already been posted. We want to keep the quality of posts high. Therefore, memes, funny videos, low-effort posts and reposts are not allowed. We prohibit giveaways because we cannot be sure that the person holding the giveaway will actually do what they promise.
5. Mark Spoilers and NSFWMake sure to mark your stuff or it may be removed. No one wants to be spoiled. Therefore, always mark spoilers. Similarly mark NSFW, in case anyone is browsing in a public space or at work.
6. No linking to piracyDon’t share it here, there are other places to find it. Discussion of piracy is fine. We don’t want us moderators or the admins of lemmy.world to get in trouble for linking to piracy. Therefore, any link to piracy will be removed. Discussion of it is of course allowed.
Authorized Regular Threads
Related communities
PM a mod to add your own
Video games
Generic
- !gaming@Lemmy.world: Our sister community, focused on PC and console gaming. Meme are allowed.
- !photomode@feddit.uk: For all your screenshots needs, to share your love for games graphics.
- !vgmusic@lemmy.world: A community to share your love for video games music
Help and suggestions
- !PatientGamers@sh.itjust.works
- !TipOfMyJoystick@retrolemmy.com
- !VideoGameSuggestions@lemmy.zip
- !Linux_Gaming@Lemmy.world - !SteamDeck@lemmy.ml
By type- !AutomationGames@lemmy.zip - !Incremental_Games@incremental.social - !LifeSimulation@lemmy.world - !CityBuilders@sh.itjust.works - !CozyGames@Lemmy.world - !CRPG@lemmy.world - !OtomeGames@ani.social - !Shmups@lemmus.org - !VisualNovels@ani.social
By games- !Baldurs_Gate_3@lemmy.world - !Cities_Skylines@lemmy.world - !CassetteBeasts@Lemmy.world - !Fallout@lemmy.world - !FinalFantasyXIV@lemmy.world - !Minecraft@Lemmy.world - !NoMansSky@lemmy.world - !Palia@Lemmy.world - !Pokemon@lemm.ee - !Skyrim@lemmy.world - !StardewValley@lemm.ee - !Subnautica2@Lemmy.world - !WorkersAndResources@lemmy.world
Language specific- !JeuxVideo@jlai.lu: French
-
A casual community to talk about LCHF/Ketogenic lifestyles, issues, benefits, difficulties, recipes, foods.
The more science focused sister community is !metabolic_health@discuss.online
Rules
- Be nice
- Stay on topic
- Don’t farm rage
- Be respectful of other diets, choices, lifestyles!!!
- No Blanket down voting - If you only come to this community to downvote its the wrong community for you
-
Welcome to the News community!
Rules:
1. Be civil___ Attack the argument, not the person. No racism/sexism/bigotry. Good faith argumentation only. This includes accusing another user of being a bot or paid actor. Trolling is uncivil and is grounds for removal and/or a community ban. Do not respond to rule-breaking content; report it and move on. ___
2. All posts should contain a source (url) that is as reliable and unbiased as possible and must only contain one link.___ Obvious right or left wing sources will be removed at the mods discretion. Supporting links can be added in comments or posted seperately but not to the post body. ___
3. No bots, spam or self-promotion.___ Only approved bots, which follow the guidelines for bots set by the instance, are allowed. ___
4. Post titles should be the same as the article used as source.___ Posts which titles don’t match the source won’t be removed, but the autoMod will notify you, and if your title misrepresents the original article, the post will be deleted. If the site changed their headline, the bot might still contact you, just ignore it, we won’t delete your post. ___
5. Only recent news is allowed.___ Posts must be news from the most recent 30 days. ___
6. All posts must be news articles.___ No opinion pieces, Listicles, editorials or celebrity gossip is allowed. All posts will be judged on a case-by-case basis. ___
7. No duplicate posts.___ If a source you used was already posted by someone else, the autoMod will leave a message. Please remove your post if the autoMod is correct. If the post that matches your post is very old, we refer you to rule 5. ___
8. Misinformation is prohibited.___ Misinformation / propaganda is strictly prohibited. Any comment or post containing or linking to misinformation will be removed. If you feel that your post has been removed in error, credible sources must be provided. ___
9. No link shorteners.___ The auto mod will contact you if a link shortener is detected, please delete your post if they are right. ___
10. Don't copy entire article in your post body___ For copyright reasons, you are not allowed to copy an entire article into your post body. This is an instance wide rule, that is strictly enforced in this community.
-
A place to discuss privacy and freedom in the digital world.
Privacy has become a very important issue in modern society, with companies and governments constantly abusing their power, more and more people are waking up to the importance of digital privacy.
In this community everyone is welcome to post links and discuss topics related to privacy.
Some Rules
- Posting a link to a website containing tracking isn’t great, if contents of the website are behind a paywall maybe copy them into the post
- Don’t promote proprietary software
- Try to keep things on topic
- If you have a question, please try searching for previous discussions, maybe it has already been answered
- Reposts are fine, but should have at least a couple of weeks in between so that the post can reach a new audience
- Be nice :)
Related communities
much thanks to @gary_host_laptop for the logo design :)
-
Carnivore
The ultimate, zero carb, elimination diet
Meat Heals.
We are focused on health and lifestyle while trying to eat zero carb bioavailable foods.
Keep being AWESOME
We welcome engaged, polite, and logical debates and questions of any type
Purpose
- lifestyle
- food
- Science
- problems
- Recipes
- Sustainability
- Regenerative lifestyle
Rules
- Be nice
- Stay on topic
- Don’t farm rage
- Be respectful of other diets, choices, lifestyles!!!
- No Blanket down voting - If you only come to this community to downvote its the wrong community for you
- No LLM generated posts . Don’t represent machine output as your own, and don’t use machines to burn human response time.
Other terms: LCHF Carnivore, Keto Carnivore, Ketogenic Carnivore, Low Carb Carnivore, Zero Carb Carnivore, Animal Based Diet, Animal Sourced Foods
Meta
If you need to block this community and the UI won’t let you, go to settings -> blocks you can add it.
-
This is a community in the spirit of “Am I The Asshole” where people can post their own bans from lemmy or reddit or whatever and get some feedback from others whether the ban was justified or not.
Sometimes one just wants to be able to challenge the arguments some mod made and this could be the place for that.
Posting Guidelines
All posts should follow this basic structure:
- Which mods/admins were being Power Tripping Bastards?
- What sanction did they impose (e.g. community ban, instance ban, removed comment)?
- Provide a screenshot of the relevant modlog entry (don’t de-obfuscate mod names).
- Provide a screenshot and explanation of the cause of the sanction (e.g. the post/comment that was removed, or got you banned).
- Explain why you think its unfair and how you would like the situation to be remedied.
Rules
- Post only about bans or other sanctions that you have received from a mod or admin.
- Don’t use private communications to prove your point. We can’t verify them and they can be faked easily.
- Don’t deobfuscate mod names from the modlog with admin powers.
- Don’t harass mods or brigade comms. Don’t word your posts in a way that would trigger such harassment and brigades.
- Do not downvote posts if you think they deserved it. Use the comment votes (see below) for that.
- You can post about power trippin’ in any social media, not just lemmy. Feel free to post about reddit or a forum etc.
- If you are the accused PTB, while you are welcome to respond, please do so within the relevant post.
Expect to receive feedback about your posts, they might even be negative.
Make sure you follow this instance’s code of conduct. In other words we won’t allow bellyaching about being sanctioned for hate speech or bigotry.
YTPB matrix channel: For real-time discussions about bastards or to appeal mod actions in YPTB itself.
Some acronyms you might see.
- PTB - Power-Tripping Bastard: The commenter agrees with you this was a PTB mod.
- YDI - You Deserved It: The commenter thinks you deserved that mod action.
- YDM new - You Deserved More: The commenter thinks you got off too lightly.
- BPR - Bait-Provoked Reaction: That mod probably overreacted in charged situation, or due to being baited.
- CLM - Clueless Mod: The mod probably just doesn’t understand how their software works.
Relevant comms
-
Welcome to the discussion of US Politics!
Rules:
- Post only links to articles, Title must fairly describe link contents. If your title differs from the site’s, it should only be to add context or be more descriptive. Do not post entire articles in the body or in the comments.
Links must be to the original source, not an aggregator like Google Amp, MSN, or Yahoo.
Example:

- Articles must be relevant to politics. Links must be to quality and original content. Articles should be worth reading. Clickbait, stub articles, and rehosted or stolen content are not allowed. Check your source for Reliability and Bias here.
- Be civil, No violations of TOS. It’s OK to say the subject of an article is behaving like a (pejorative, pejorative). It’s NOT OK to say another USER is (pejorative). Strong language is fine, just not directed at other members. Engage in good-faith and with respect! This includes accusing another user of being a bot or paid actor. Trolling is uncivil and is grounds for removal and/or a community ban.
- No memes, trolling, or low-effort comments. Reposts, misinformation, off-topic, trolling, or offensive. Similarly, if you see posts along these lines, do not engage. Report them, block them, and live a happier life than they do. We see too many slapfights that boil down to “Mom! He’s bugging me!” and “I’m not touching you!” Going forward, slapfights will result in removed comments and temp bans to cool off.
- Vote based on comment quality, not agreement. This community aims to foster discussion; please reward people for putting effort into articulating their viewpoint, even if you disagree with it.
- No hate speech, slurs, celebrating death, advocating violence, or abusive language. This will result in a ban. Usernames containing racist, or inappropriate slurs will be banned without warning
We ask that the users report any comment or post that violate the rules, to use critical thinking when reading, posting or commenting. Users that post off-topic spam, advocate violence, have multiple comments or posts removed, weaponize reports or violate the code of conduct will be banned.
All posts and comments will be reviewed on a case-by-case basis. This means that some content that violates the rules may be allowed, while other content that does not violate the rules may be removed. The moderators retain the right to remove any content and ban users.
That’s all the rules!
Civic Links
• Congressional Awards Program
• Library of Congress Legislative Resources
• U.S. House of Representatives
Partnered Communities:
• News
-
Welcome to Movies, a community for discussing movies, film news, box office, and more! We want this to be a place for members to feel safe to discuss and share everything they love about movies and movie related things. Please feel free to take part and help our community grow!
Related Communities:
!books@lemmy.world - Discussing books and book-related things.
!comicbooks@lemmy.world - A place to discuss comic books of all types.
!marvelstudios@lemmy.world - LW’s home for all things MCU.
While posting and commenting in this community, you must abide by the Lemmy.World Terms of Service: legal.lemmy.world/tos/
-
Posts or comments that are homophobic, transphobic, racist, sexist, ableist, or advocating violence will be removed.
-
Be civil: disagreements happen, but that doesn’t provide the right to personally insult others.
-
Spam, self promotion, trolling, and bots are not allowed
-
Shitposts and memes are allowed until they prove to be a problem.
Regarding spoilers; Please put “(Spoilers)” in the title of your post if you anticipate spoilers, as we do not currently have a spoiler tag available. If your post contains an image that could be considered a spoiler, please mark the thread as NSFW so the image gets blurred. As far as how long to wait until the post is no longer a spoiler, please just use your best judgement. Everyone has a different idea on this, so we don’t want to make any hard limits.
Please use spoiler tags whenever commenting a spoiler in a non-spoiler thread. Most of the Lemmy clients don’t support this but we want to get into the habit as clients will be supporting in the future.
Failure to follow these guidelines will result in your post/comment being removed and/or more severe actions. All posts and comments will be reviewed on a case-by-case basis. This means that some content that violates the rules may be allowed, while other content that does not violate the rules may be removed. The moderators retain the right to remove any content and ban users. We ask that the users report any comment or post that violates the rules, and to use critical thinking when reading, posting or commenting.
-
-
YSK - for all the things that can make your life easier!
The rules for posting and commenting, besides the rules defined here for lemmy.world, are as follows:
Rules (interactive)
Rule 1- All posts must begin with YSK.All posts must begin with YSK. If you’re a Mastodon user, then include YSK after @youshouldknow. This is a community to share tips and tricks that will help you improve your life. _____________
:::spoiler Rule 2- Your post body text must include the reason “Why” YSK:
**In your post’s text body, you must include the reason “Why” YSK: It’s helpful for readability, and informs readers about the importance of the content. **
:::
:::spoiler Rule 3- Do not seek mental, medical and professional help here.
Do not seek mental, medical and professional help here. Breaking this rule will not get you or your post removed, but it will put you at risk, and possibly in danger.
:::
:::spoiler Rule 4- No self promotion or upvote-farming of any kind.
That’s it.
:::
:::spoiler Rule 5- No baiting or sealioning or promoting an agenda.
Posts and comments which, instead of being of an innocuous nature, are specifically intended (based on reports and in the opinion of our crack moderation team) to bait users into ideological wars on charged political topics will be removed and the authors warned - or banned - depending on severity.
:::
:::spoiler Rule 6- Regarding non-YSK posts.
Provided it is about the community itself, you may post non-YSK posts using the [META] tag on your post title.
:::
:::spoiler Rule 7- You can’t harass or disturb other members.
If you harass or discriminate against any individual member, you will be removed.
If you are a member, sympathizer or a resemblant of a movement that is known to largely hate, mock, discriminate against, and/or want to take lives of a group of people and you were provably vocal about your hate, then you will be banned on sight.
For further explanation, clarification and feedback about this rule, you may follow this link.
:::
:::spoiler Rule 8- All comments should try to stay relevant to their parent content.
:::
:::spoiler Rule 9- Reposts from other platforms are not allowed.
Let everyone have their own content.
:::
:::spoiler Rule 10- The majority of bots aren’t allowed to participate here.
Unless included in our Whitelist for Bots, your bot will not be allowed to participate in this community. To have your bot whitelisted, please contact the moderators for a short review.
:::
:::spoiler Rule 11- Posts must actually be true: Disiniformation, trolling, and being misleading will not be tolerated. Repeated or egregious attempts will earn you a ban. This also applies to filing reports: If you continually file false reports YOU WILL BE BANNED! We can see who reports what, and shenanigans will not be tolerated. We are not here to ban people who said something you don’t like.
If you file a report, include what specific rule is being violated and how.
:::
Partnered Communities:
You can view our partnered communities list by following this link. To partner with our community and be included, you are free to message the moderators or comment on a pinned post.
Community Moderation
For inquiry on becoming a moderator of this community, you may comment on the pinned post of the time, or simply shoot a message to the current moderators.
Credits
Our icon(masterpiece) was made by @clen15!
-
A community for discussing events around the World
Rules:
-
Rule 1: posts have the following requirements:
- Post news articles only
- Video links are NOT articles and will be removed.
- Title must match the article headline
- Not United States Internal News
- Recent (Past 30 Days)
- Screenshots/links to other social media sites (Twitter/X/Facebook/Youtube/reddit, etc.) are explicitly forbidden, as are link shorteners.
-
Rule 2: Do not copy the entire article into your post. The key points in 1-2 paragraphs is allowed (even encouraged!), but large segments of articles posted in the body will result in the post being removed. If you have to stop and think “Is this fair use?”, it probably isn’t. Archive links, especially the ones created on link submission, are absolutely allowed but those that avoid paywalls are not.
-
Rule 3: Opinions articles, or Articles based on misinformation/propaganda may be removed.
-
Rule 4: Posts or comments that are homophobic, transphobic, racist, sexist, anti-religious, or ableist will be removed. “Ironic” prejudice is just prejudiced.
-
Posts and comments must abide by the lemmy.world terms of service UPDATED AS OF OCTOBER 19 2025
-
Rule 5: Keep it civil. It’s OK to say the subject of an article is behaving like a (pejorative, pejorative). It’s NOT OK to say another USER is (pejorative). Strong language is fine, just not directed at other members. Engage in good-faith and with respect! This includes accusing another user of being a bot or paid actor. Trolling is uncivil and is grounds for removal and/or a community ban.
Similarly, if you see posts along these lines, do not engage. Report them, block them, and live a happier life than they do. We see too many slapfights that boil down to “Mom! He’s bugging me!” and “I’m not touching you!” Going forward, slapfights will result in removed comments and temp bans to cool off.
-
Rule 6: Memes, spam, other low effort posting, reposts, misinformation, advocating violence, off-topic, trolling, offensive, regarding the moderators or meta in content may be removed at any time.
-
Rule 7: We didn’t USED to need a rule about how many posts one could make in a day, then someone posted NINETEEN articles in a single day. Not comments, FULL ARTICLES. If you’re posting more than say, 10 or so, consider going outside and touching grass. We reserve the right to limit over-posting so a single user does not dominate the front page.
We ask that the users report any comment or post that violate the rules, to use critical thinking when reading, posting or commenting. Users that post off-topic spam, advocate violence, have multiple comments or posts removed, weaponize reports or violate the code of conduct will be banned.
All posts and comments will be reviewed on a case-by-case basis. This means that some content that violates the rules may be allowed, while other content that does not violate the rules may be removed. The moderators retain the right to remove any content and ban users.
Lemmy World Partners
News !news@lemmy.world
Politics !politics@lemmy.world
World Politics !globalpolitics@lemmy.world
Recommendations
For Firefox users, there is media bias / propaganda / fact check plugin.
addons.mozilla.org/…/media-bias-fact-check/
- Consider including the article’s mediabiasfactcheck.com/ link
-
-
A loosely moderated place to ask open-ended questions
If your post meets the following criteria, it’s welcome here!
- Open-ended question
- Not offensive: at this point, we do not have the bandwidth to moderate overtly political discussions. Assume best intent and be excellent to each other.
- Not regarding using or support for Lemmy: context, see the list of support communities and tools for finding communities below
- Not ad nauseam inducing: please make sure it is a question that would be new to most members
- An actual topic of discussion
Looking for support?
Looking for a community?
- Lemmyverse: community search
- sub.rehab: maps old subreddits to fediverse options, marks official as such
- !lemmy411@lemmy.ca: a community for finding communities
~Icon~ ~by~ ~@Double_A@discuss.tchncs.de~
-
Welcome to the Massachusetts sublemmy!
A place to connect, share, and discuss all things Massachusetts. Whether you’re a local, a visitor, or just curious about the Bay State, this community is here for you.
Feel free to post about local events, news, history, landmarks, university events, politics, and anything else related to Massachusetts. Let’s celebrate the rich culture, diverse communities, and stunning landscapes that make this state so special. Please remember to follow our sublemmy rules, be respectful towards each other, and keep discussions civil. Let’s foster a positive and inclusive environment where everyone feels welcome.
Explore the wonders of Massachusetts with us and join the conversation. Welcome aboard!
-
Nice photographs with nice beers
Rules:
- All photos must include a beer and a view. No videos, no cocktails.
- Views are of nature, a cityscape, or an event. It’s ok to include people and pets in the picture, but should not be the primary view.
- Please include location in the title.
- SFW Only.
-
Welcome to Programmer Humor!
This is a place where you can post jokes, memes, humor, etc. related to programming!
For sharing awful code theres also Programming Horror.
Rules
- Keep content in english
- No advertisements
- Posts must be related to programming or programmer topics
-
A place to share screenshots of Microblog posts, whether from Mastodon, tumblr,
TwitterX, KBin, Threads or elsewhere.Created as an evolution of White People Twitter and other tweet-capture subreddits.
Rules:
- Please put at least one word relevant to the post in the post title.
- Be nice.
- No advertising, brand promotion or guerilla marketing.
- Posters are encouraged to link to the toot or tweet etc in the description of posts.
Related communities:
- !whitepeopletwitter@sh.itjust.works
- !curatedtumblr@sh.itjust.works
-
Rules:
1… Please mark original photos with [OC] in the title if you’re the photographer
2…Pictures containing a politician from any country or planet are prohibited, this is a community voted on rule.
3… Image must be a photograph, no AI or digital art.
4… No NSFW/Cosplay/Spam/Trolling images.
5… Be civil. No racism or bigotry.
Photo of the Week Rule(s):
1… On Fridays, the most upvoted original, marked [OC], photo posted between Friday and Thursday will be the next week’s banner and featured photo.
2… The weekly photos will be saved for an end of the year run off.
Instance-wide rules always apply. mastodon.world/about
-
Welcome to Political Humor!
Rules:
- Be excellent to each other.
- No harassment.
- No sexism, racism or bigotry.
- All arguments should be made in good faith.
- No misinformation. Be prepared to back up your factual claims with evidence.
- All posts should relate to politics and be of a humorous nature.
- No bots, spam or self-promotion.
- If you want to run a bot, ask first.
- Site wide rules apply.
- Have fun.
-
-
Vintage gaming community.
Rules:
- Be kind.
- No spam, AI slop, or soliciting for money.
- No racism or other bigotry allowed.
- Obviously nothing illegal.
If you see these please report them.
-
Welcome to a little slice of culinary heaven where we share photos of our favorite dishes, from savory succulent sausages to delicious and delectable desserts. Made it yourself? We’d love to hear your recipe!
Rules:
1. BE KIND
Food should bring people together, not tear them apart. Think of the human on the other side of the screen, and don’t troll, harass, engage in bigotry, or otherwise make others uncomfortable with your words.
2. NO ADVERTISING
This community is for sharing pictures of awesome food, not a platform to advertise.
3. NO MEMES
4. PICTURES SHOULD BE OF FOOD
Preferably good, high quality pictures of good looking grub; for pictures of terrible food, see !shittyfoodporn@lemmy.ca
Other Cooking Communities:
Be sure to check out these other awesome and fun food related communities!
!cooking@lemmy.world - A general communty about all things cooking.
!sousvide@lemmy.world - All about sous vide precision cooking.
!koreanfood@lemmy.world - Celebrating Korean cuisine!
-
A place with minimal rules for stuff that makes you go awww! Feel free to post pics, gifs, or videos of cats, dogs, babies, or anything cute and remember to be kind to others.
AI posts must be labeled [AI] in the title and are limited to one per week.
While posting and commenting in this community, you must abide by instance-wide rules: mastodon.world/about
- No racism or bigotry.
- Be civil: disagreements happen, but thatdoes not provide the right to personally insult others.
- No SPAM posting.
- No trolling of others.
-
Welcome
We’re not The Onion! Not affiliated with them in any way! Not operated by them in any way! All the news here is real!
The Rules
Posts must be:
- Links to news stories from…
- …credible sources, with…
- …their original headlines, that…
- …would make people who see the headline think, “That has got to be a story from The Onion, America’s Finest News Source.”
Please also avoid duplicates.
Comments and post content must abide by the server rules for Lemmy.world and generally abstain from trollish, bigoted, or otherwise disruptive behavior that makes this community less fun for everyone.
And that’s basically it!
-
Welcome to c/boston,
A community for all things related to Boston, Massachusetts. Whether you’re a local, a visitor, or just interested in the city, this is the place to discuss, share, and connect with fellow Bostonians.
Greater Boston area discussion is welcome here.
Rules:
Be respectful: Treat others with respect and courtesy. Personal attacks, trolling, and harassment will not be tolerated.
Stay on topic: Keep discussions relevant to Boston and its surrounding areas.
-
Welcome to Lemmy Shitpost. Here you can shitpost to your hearts content.
Anything and everything goes. Memes, Jokes, Vents and Banter. Though we still have to comply with lemmy.world instance rules. So behave!
Rules:
1. Be Respectful___ Refrain from using harmful language pertaining to a protected characteristic: e.g. race, gender, sexuality, disability or religion. Refrain from being argumentative when responding or commenting to posts/replies. Personal attacks are not welcome here. …
2. No Illegal Content___ Content that violates the law. Any post/comment found to be in breach of common law will be removed and given to the authorities if required. That means: -No promoting violence/threats against any individuals -No CSA content or Revenge Porn -No sharing private/personal information (Doxxing) …
3. No Spam___ Posting the same post, no matter the intent is against the rules. -If you have posted content, please refrain from re-posting said content within this community. -Do not spam posts with intent to harass, annoy, bully, advertise, scam or harm this community. -No posting Scams/Advertisements/Phishing Links/IP Grabbers -No Bots, Bots will be banned from the community. …
4. No Porn/ExplicitContent ___ -Do not post explicit content. Lemmy.World is not the instance for NSFW content. -Do not post Gore or Shock Content. …
5. No Enciting Harassment,Brigading, Doxxing or Witch Hunts ___ -Do not Brigade other Communities -No calls to action against other communities/users within Lemmy or outside of Lemmy. -No Witch Hunts against users/communities. -No content that harasses members within or outside of the community. …
6. NSFW should be behind NSFW tags.___ -Content that is NSFW should be behind NSFW tags. -Content that might be distressing should be kept behind NSFW tags.
…
If you see content that is a breach of the rules, please flag and report the comment and a moderator will take action where they can.
Also check out:
Partnered Communities:
1.Memes
10.LinuxMemes (Linux themed memes)
Reach out to
All communities included on the sidebar are to be made in compliance with the instance rules. Striker
-
↳ Our family Communities:
***➰#Music***> Music.world - !music@lemmy.world > Jazz -!jazz@lemmy.world > Album Art Porn - !albumartporn@lemmy.world > Fake Album Covers - !fakealbumcovers@lemm.ee > Obscure Music - !ObscureMusic@lemm.ee > Vinyl and LP’s - !vinyl@lemmy.world > Electronic Dance Music - !edm@reddthat.com > 60’s Music - !60smusic@lemmy.world > 70’s Music - !70smusic@lemmy.world > 80’s Music - !80smusic@lemmy.world > 90’s Music - !90smusic@lemmy.world
-
Welcome to General Memes
Memes for the masses, chuckles for the chosen.
Rule 1: Be Civil, Not CruelWe’re here for laughs, not fights.
Rule 2: No Forbidden Formats
- No harassment, dogpiling, or brigading
- No bigotry (transphobia, racism, sexism, etc.)
- Keep it light — argue in the comments, not with insults
Not every image deserves immortality on the memmlefield. That means:
- No spam or scams
- No porn or sexually explicit content
- No illegal content (seriously, don’t ruin the fun)
- NSFW memes must be properly tagged
If you see a post that breaks the rules, report it so the mods can take care of it.
Otherwise consider this your call to duty. Get posting or laughing. Up to you
-
Welcome to LW Cooking, a community for discussing all things related to food and cooking! We want this to be a place for members to feel safe to discuss and share everything they love about the culinary arts. Please feel free to take part and help our community grow!
Taken a nice photo of your creation? We highly encourage sharing with our friends over at !foodporn@lemmy.world.
Posts in this community must be food/cooking related. Recipes for dishes you’ve made and post picture of are encouraged but are not a requirement. Posts of food you are enjoyed or just think like food are welcomed as well.
Posts can optionally be tagged. We would like the use and number of tags to grow organically. Feel free to use a tag that isn’t listed if you think it makes sense to do so. We encourage using tags to help organize and make browsing easier, but you don’t have to use them if you don’t want to.
TAGS:
- [QUESTION] - For questions about cooking.
- [RECIPE} - Share a recipe of your own, or link one.
- [MEME] - Food related meme or funny post.
- [DISCUSSION] - For general culinary discussion.
- [TIP] - Helpful cooking tips.
FORMAT:
[QUESTION] What are your favorite spices to use in soups?
Other Cooking Communities:
!bbq@lemmy.world - Lemmy.world’s home for BBQ.
!foodporn@lemmy.world - Showcasing your best culinary creations.
!sousvide@lemmy.world - All things sous vide precision cooking.
!koreanfood@lemmy.world - Celebrating Korean cuisine!
While posting and commenting in this community, you must abide by the Lemmy.World Terms of Service: legal.lemmy.world/tos/
- Posts or comments that are homophobic, transphobic, racist, sexist, ableist, or advocating violence will be removed.
- Be civil: disagreements happen, but that doesn’t provide the right to personally insult others.
- Spam, self promotion, trolling, and bots are not allowed
- Shitposts and memes are allowed until they prove to be a problem.
Failure to follow these guidelines will result in your post/comment being removed and/or more severe actions. All posts and comments will be reviewed on a case-by-case basis. This means that some content that violates the rules may be allowed, while other content that does not violate the rules may be removed. The moderators retain the right to remove any content and ban users. We ask that the users report any comment or post that violates the rules, and to use critical thinking when reading, posting or commenting.
-
“We did it, Patrick! We made a technological breakthrough!”
A place for all those who loathe AI to discuss things, post articles, and ridicule the AI hype. Proud supporter of working people. And proud booer of SXSW 2024.
AI, in this case, refers to LLMs, GPT technology, and anything listed as “AI” meant to increase market valuations.
-
DROID DOES
Welcome to the droidymcdroidface-iest, Lemmyest (Lemmiest), test, bestest, phoniest, pluckiest, snarkiest, and spiciest Android community on Lemmy (Do not respond)! Here you can participate in amazing discussions and events relating to all things Android.
The rules for posting and commenting, besides the rules defined here for lemmy.world, are as follows:
Rules
1. All posts must be relevant to Android devices/operating system.
2. Posts cannot be illegal or NSFW material.
3. No spam, self promotion, or upvote farming. Sources engaging in these behavior will be added to the Blacklist.
4. Non-whitelisted bots will be banned.
5. Engage respectfully: Harassment, flamebaiting, bad faith engagement, or agenda posting will result in your posts being removed. Excessive violations will result in temporary or permanent ban, depending on severity.
6. Memes are not allowed to be posts, but are allowed in the comments.
7. Posts from clickbait sources are heavily discouraged. Please de-clickbait titles if it needs to be submitted.
8. Submission statements of any length composed of your own thoughts inside the post text field are mandatory for any microblog posts, and are optional but recommended for article/image/video posts.
Community Resources:
We are Android girls*,
In our Lemmy.world.
The back is plastic,
It’s fantastic.
*Well, not just girls: people of all gender identities are welcomed here.
Our Partner Communities:
!android@lemmy.ml
-
Rules:
Be a decent person, don’t post hate.Other Great Communities:
* !europe@lemmy.dbzer0.com
* !canada@lemmy.caRules
Be excellent to each other
-
News and discussion related to Ukraine
Community Rules
🇺🇦 Sympathy for enemy combatants is prohibited.
🌻🤢No content depicting extreme violence or gore.
💥Posts containing combat footage should include [Combat] in title
🚷Combat videos containing any footage of a visible human involved must be flagged NSFW
**❗ Server Rules**1. Remember the human! (no harassment, threats, etc.) 2. No racism or other discrimination 3. No Nazis, QAnon or similar 4. No porn 5. No ads or spam (includes charities) 6. No content against Finnish law
💳 Defense Aid 💥
💳 Humanitarian Aid ⚕️⛑️
🪖 Volunteer with the International Legionnaires
See also:
-
An unofficial chapter of the popular Dull Men’s Club.
1. Relevant commentary on your own dull life. Posts should be about your own dull, lived experience. This is our most important rule. Direct questions, random thoughts, comment baiting, advice seeking, many uses of “discuss” rarely comply with this rule.
2. Original, Fresh, Meaningful Content.
3. Avoid repetitive topics.
4. This is not a search engine
Use a search engine, a tradesperson, Reddit, friends, a specialist Facebook group, apps, Wikipedia, an AI chat, a reverse image search etc. to answer simple questions or identify objects. Also see rule 1, “comment baiting”.There are a number of content specific communities with subject matter experts who can help you.
Some other communities to consider before posting:
5. Keep it dull. If it puts us to sleep, it’s on the right track. Examples of likely not dull: jokes, gross stuff (including toes), politics, religion, royalty, illness or injury, killing things for fun, or promotional content. Feel free to post these elsewhere.
6. No hate speech, sexism, or bullying No sexism, hate speech, degrading or excessively foul language, or other harmful language. No othering or dehumanizing of anyone or negativity towards any gender identity.
7. Proofread before posting. Use good grammar and punctuation. Avoid useless phrases. Some examples: - starting a post with “So” - starting a post with pointless phrases, like “I hope this is allowed” or “this is my first post” Only share good quality, cropped images. Do not share screenshots of images; share the original image.
.
-
Post memes here.
A meme is an idea, behavior, or style that spreads by means of imitation from person to person within a culture and often carries symbolic meaning representing a particular phenomenon or theme.
An Internet meme or meme, is a cultural item that is spread via the Internet, often through social media platforms. The name is by the concept of memes proposed by Richard Dawkins in 1972. Internet memes can take various forms, such as images, videos, GIFs, and various other viral sensations.
- Wait at least 2 months before reposting
- No explicitly political content (about political figures, political events, elections and so on), !politicalmemes@lemmy.ca can be better place for that
- Use NSFW marking accordingly
Laittakaa meemejä tänne.
- Odota ainakin 2 kuukautta ennen meemin postaamista uudelleen
- Ei selkeän poliittista sisältöä (poliitikoista, poliittisista tapahtumista, vaaleista jne) parempi paikka esim. !politicalmemes@lemmy.ca
- Merkitse K18-sisältö tarpeen mukaan
-
What did you learn today? Share it with us!
We learn something new every day. This is a community dedicated to informing each other and helping to spread knowledge.
The rules for posting and commenting, besides the rules defined here for lemmy.world, are as follows:
Rules (interactive)
Rule 1- All posts must begin with TIL. Linking to a source of info is optional, but highly recommended as it helps to spark discussion.** Posts must be about an actual fact that you have learned, but it doesn’t matter if you learned it today. See Rule 6 for all exceptions.** _____________
:::spoiler Rule 2- Your post subject cannot be illegal or NSFW material.
Your post subject cannot be illegal or NSFW material. You will be warned first, banned second.
:::
:::spoiler Rule 3- Do not seek mental, medical and professional help here.
Do not seek mental, medical and professional help here. Breaking this rule will not get you or your post removed, but it will put you at risk, and possibly in danger.
:::
:::spoiler Rule 4- No self promotion or upvote-farming of any kind.
That’s it.
:::
:::spoiler Rule 5- No baiting or sealioning or promoting an agenda.
Posts and comments which, instead of being of an innocuous nature, are specifically intended (based on reports and in the opinion of our crack moderation team) to bait users into ideological wars on charged political topics will be removed and the authors warned - or banned - depending on severity.
:::
:::spoiler Rule 6- Regarding non-TIL posts.
Provided it is about the community itself, you may post non-TIL posts using the [META] tag on your post title.
:::
:::spoiler Rule 7- You can’t harass or disturb other members.
If you vocally harass or discriminate against any individual member, you will be removed.
Likewise, if you are a member, sympathiser or a resemblant of a movement that is known to largely hate, mock, discriminate against, and/or want to take lives of a group of people, and you were provably vocal about your hate, then you will be banned on sight.
For further explanation, clarification and feedback about this rule, you may follow this link.
:::
:::spoiler Rule 8- All comments should try to stay relevant to their parent content.
:::
:::spoiler Rule 9- Reposts from other platforms are not allowed.
Let everyone have their own content.
:::
:::spoiler Rule 10- Majority of bots aren’t allowed to participate here.
Unless included in our Whitelist for Bots, your bot will not be allowed to participate in this community. To have your bot whitelisted, please contact the moderators for a short review.
:::
Partnered Communities
You can view our partnered communities list by following this link. To partner with our community and be included, you are free to message the moderators or comment on a pinned post.
Community Moderation
For inquiry on becoming a moderator of this community, you may comment on the pinned post of the time, or simply shoot a message to the current moderators.
-
A place to discuss problems of car centric infrastructure or how it hurts us all. Let’s explore the bad world of Cars!
Rules
1. Be CivilYou may not agree on ideas, but please do not be needlessly rude or insulting to other people in this community.
2. No hate speechDon’t discriminate or disparage people on the basis of sex, gender, race, ethnicity, nationality, religion, or sexuality.
3. Don't harass peopleDon’t follow people you disagree with into multiple threads or into PMs to insult, disparage, or otherwise attack them. And certainly don’t doxx any non-public figures.
4. Stay on topicThis community is about cars, their externalities in society, car-dependency, and solutions to these.
5. No repostsDo not repost content that has already been posted in this community.
Moderator discretion will be used to judge reports with regard to the above rules.
Posting Guidelines
In the absence of a flair system on lemmy yet, let’s try to make it easier to scan through posts by type in here by using tags:
- [meta] for discussions/suggestions about this community itself
- [article] for news articles
- [blog] for any blog-style content
- [video] for video resources
- [academic] for academic studies and sources
- [discussion] for text post questions, rants, and/or discussions
- [meme] for memes
- [image] for any non-meme images
- [misc] for anything that doesn’t fall cleanly into any of the other categories
Recommended communities:
- !yimby@lemmy.world
-
A place to talk about and post pictures of cats
-
Hello fellow Far Side fans!
About this community and how I post the comic strip… Many moons ago, I would ask my Dad to save the newspaper for me everyday so I could read my favorite comic strips and one of those was The Far Side. These days of course you find just about anything online including www.thefarside.com where they post several comics a day and I repost them here. Just to note, the date you see in my posts is not the initial release date, but the date they were posted on the website.
The Far Side is a single-panel comic created by Gary Larson and syndicated by Chronicle Features and then Universal Press Syndicate, which ran from December 31, 1979, to January 1, 1995 (when Larson retired as a cartoonist). Its surrealistic humor is often based on uncomfortable social situations, improbable events, an anthropomorphic view of the world, logical fallacies, impending bizarre disasters, (often twisted) references to proverbs, or the search for meaning in life… Read more: en.wikipedia.org/wiki/The_Far_Side
Hope you enjoy and feel free to contribute to the community with art, cool stuff about the author, tattoos, toys and anything else, as long it’s The Far Side!
Ps. Sub to all my comic strip communities:
Bello Bear !BelloBear@lemmy.world lemmy.world/c/bellobearofficial
Bloom County !bloomcounty@lemm.ee lemm.ee/c/bloomcounty
Calvin and Hobbes !calvinandhobbes@lemmy.world lemmy.world/c/calvinandhobbes
Cyanide and Happiness !cyanideandhappiness lemm.ee/c/cyanideandhappiness
Garfield !garfield@lemmy.world lemmy.world/c/garfield
The Far Side !thefarside@sh.itjust.works lemmy.world/c/thefarside@sh.itjust.works
Fine print: All comics I post are freely available online. In no way am I claiming ownership, copyright or anything else. This is a not for profit community, we just want to enjoy our comics, thank you.
-
Seize the Memes of Production
An international (English speaking) socialist Lemmy community free of the “ML” influence of instances like lemmy.ml and lemmygrad. This is a place for undogmatic shitposting and memes from a progressive, anti-capitalist and truly anti-imperialist perspective, regardless of specific ideology.
-
A community discussing turntables, vinyl and the art of listening to high-fidelity music on spinning platters.
You might also want to check out !albumartporn@lemmy.world.
-
Be sure to follow the rule before you head out.
Rule: You must post before you leave.
Other rules
Behavior rules:
- No bigotry (transphobia, racism, etc…)
- No genocide denial
- No support for authoritarian behaviour (incl. Tankies)
- No namecalling
- Accounts from lemmygrad.ml, threads.net, or hexbear.net are held to higher standards
- Other things seen as cleary bad
Posting rules:
- No AI generated content (DALL-E etc…)
- No advertisements
- No gore / violence
- Mutual aid posts are not allowed
NSFW: NSFW content is permitted but it must be tagged and have content warnings. Anything that doesn’t adhere to this will be removed. Content warnings should be added like: [penis], [explicit description of sex]. Non-sexualized breasts of any gender are not considered inappropriate and therefore do not need to be blurred/tagged.
If you have any questions, feel free to contact us on our matrix channel or email.
Other 196’s:
- !196@lemmy.world
- !onehundredninetysix@lemmy.blahaj.zone
-
Southern Alberta Beer, Small Craft Brewery Info!
-
A place for for news, discussion, memes, and links criticizing capitalism and advancing viewpoints that challenge liberal capitalist ideology. That means any support for any liberal capitalist political party (like the Democrats) is strictly prohibited.
A zero-tolerance policy for bigotry of any kind. Failure to respect this will result in a ban.
RULES:
1 Understand the left starts at anti-capitalism.
2 No Trolling
3 No capitalist apologia, anti-socialism, or liberalism, liberalism is in direct conflict with the left. Support for capitalism or for the parties or ideologies that uphold it are not welcome or tolerated.
4 No imperialism, conservatism, reactionism or Zionism, lessor evil rhetoric. Dismissing 3rd party votes or ‘wasted votes on 3rd party’ is lessor evil rhetoric.
5 No bigotry, no racism, sexism, antisemitism, homophobia, transphobia, ableism, or any type of prejudice.
6 Be civil in comments and no accusations of being a bot, ‘paid by Putin,’ Tankie, etc. This includes instance shaming.
-
About
An alliance among all who oppose Donald Trump’s actions, positions, cabinet, supporters, policies, or motives. This alliance includes anyone from the left or the right; anyone from any religion or lack thereof; anyone from any country or state; any man, woman or child.
Rules
-No pro-Trump posts or comments
-No off topic posts
-Be civil
-No trolling
-Follow Lemmy terms of service
Social Media
Other Communities
!desantisthreatensusa@lemmy.world
!antifascism@midwest.social
!politicus@kbin.social

-
This is a page for anything that’s amusing, interesting, outrageous, or profound.
♦ ♦ ♦
RULES
❶ Each player gets six cards, except the player on the dealer’s right, who gets seven.
❷ Posts, comments, and participants must be amusing, interesting, outrageous, or profound.
❸ This page uses Reverse Lemmy-Points™, or ‘bad karma’. Please downvote all posts and comments.
❹ Posts, comments, and participants that are not amusing, interesting, outrageous, or profound will be removed.
❺ This is a non-smoking page. If you must smoke, please click away and come back later.
❻ Don’t be a dick.
Please also abide by the instance rules.
♦ ♦ ♦
Can’t get enough? Visit my blog.
♦ ♦ ♦
Please consider donating to Lemmy and Lemmy.World.
$5 a month is all they ask — an absurdly low price for a Lemmyverse of news, education, entertainment, and silly memes.
-
Place to post pics from old movies and discuss everything about it
-
Welcome to the Fediverse’s Community for all things Classic Rock!
Join fellow music enthusiasts as we celebrate the timeless sounds, iconic bands and unforgettable melodies that have shaped generations. Share your love for the legends, discover the hidden gems, and connect with fellow fans!
If your song is old enough to drink, share it here! (Released on or before January 2004)
Share links, videos, bios, photos, etc.
Community Guidelines- Don’t be a dick. - No bigotry - including racism, sexism, ableism, homophobia, transphobia, or xenophobia. - Be respectful, especially when disagreeing. Everyone should feel welcome here. - No porn. - No Ads / Spamming.
Check out other Lemmy music communities
!gratefuldead@lemmy.world !radiolemmy@lemm.ee !music@lemmy.world !AlternativeNation@lemmy.world !90smusic@lemmy.world !80smusic@lemmy.world !70smusic@lemmy.world !60smusic@lemmy.world
-
Anything related to the NASA (National Aeronautics and Space Administration); the latest news, events, current and future missions, and more.
Note: This community is an unofficial forum and is unaffiliated with NASA or the U.S. government.
Rules
- Be respectful and inclusive.
- No harassment, hate speech, or trolling.
- Engage in constructive discussions.
- Share relevant content.
- Follow guidelines and moderators’ instructions.
- Use appropriate language and tone.
- Report violations.
- Foster a continuous learning environment.
-
!egg_irl
!egg_irl is for widely relatable memes about questioning one’s gender or being an egg (a trans person in denial) as well as other eggy topics.
If you are looking for a place to discuss something specific to you or especially if you need help or are in crisis, we have communities and resources that can support you linked at the bottom of this sidebar.
General Rules:
-
No bigotry.
-
No spam, bots, or vote farming.
Rules on Content:
-
No reposts.
-
No personal-life posts, bingo cards, quizzes, selfies, “trans/not trans” lists, picrew, or non-memes.
-
No visible names or usernames.
-
Do not post or link to pornography.
Rules on Post Titles and Tags:
-
Posts must be titled “egg_irl”. An emoji or two is OK, but they have to be between “egg” and “irl”.
-
Posts that assume the viewer’s gender and/or contain potentially triggering content must be spoilered and tagged at the beginning of the post title. Example content-warning tags that you can copy include the following:
[CW: Assumes Viewer is Transmasc][CW: Assumes Viewer is Transfem][CW: Assumes Viewer is Nonbinary][CW: Transphobia][CW: Violence][CW: Weapons/Firearms][CW: Disturbing Imagery][CW: Fictional Egging]
-
You may optionally include other tags, such as:
[Transmasc Meme][Transfem Meme][Nonbinary Meme][Gender-Nonspecific Meme]
Rules on Post Text:
-
If possible, include an image description for accessibility.
-
Add sources for art.
Rules on Comments
-
If a post is tagged with a specific gender identity, keep the conversation centered on that identity.
-
You must follow the Egg Prime Directive. You may not push or coerce people into identifying or not identifying a certain way. You must respect them as the gender they claim to identify as. In addition it is extremely in poor taste to make assumptions about other people’s identities based on external factors, we understand it cannot be helped but it is best not to as it can affect the way you treat others in noticeable ways. Read more about this decision here.
-
No Ewwphoria posts. Posts which contain misogyny, misandry, transmisogyny, transmisandry, or enbyphobia for the purpose of expressing euphoria are not allowed here. At best they bring anger to others, and at worst they may trigger people’s dysphoria. People who create such posts will have them removed and may be banned at moderator discretion.
Recommendations:
We strongly encourage you to include your pronouns in your account bio so that others know how to refer to you without misgendering you. If you’re questioning or unsure of your pronouns, that’s totally cool—just say so.
Sibling Meme Communities
- !traa (or search for https://lemmy.ca/c/traaaaaaannnnnnnnnns in your instance if the link doesn’t work)
Sibling Non-Meme Communities
- !transgender (or search for https://lemmy.ml/c/transgender in your instance if the link doesn’t work)
- !trans (or search for https://lemmy.blahaj.zone/c/trans in your instance if the link doesn’t work)
- !ftm (and transmasc) (or search for https://lemmy.blahaj.zone/c/ftm in your instance if the link doesn’t work)
- !mtf (and transfem) (or search for https://lemmy.blahaj.zone/c/mtf in your instance if the link doesn’t work)
- !nonbinary@lemmy.one (or search for https://lemmy.one/c/nonbinary in your instance if the link doesn’t work)
- !lgbtq_plus@beehaw.org (or search for https://beehaw.org/c/lgbtq_plus in your instance if the link doesn’t work)
- !lgbtq_plus@lemmy.blahaj.zone (or search for https://lemmy.blahaj.zone/c/lgbtq_plus in your instance if the link doesn’t work)
Community Resources:
- The Trevor Project / 1-866-488-7386 — A US-based crisis prevention and intervention hotline and community
- TransLifeLine / 1-877-565-8860 — A US-based trans peer support hotline
- The Gender Dysphoria Bible — An in-depth explanation of the different types of gender dysphoria
- Trans Resources — A directory of resources for trans, non-binary, and gender-non-conforming people
- LGBTQ+ Healthcare Directory — A directory of LGBTQ+ accepting Healthcare providers
- Trans Resistance Network — A US-based mutual-aid organization to help trans people facing state violence and legal discrimination
- TLDEF’s Trans Health Project — Advice about insurance claims for trans healthcare procedures
- TransLifeLine’s ID change Library — A comprehensive guide to changing your name on any US legal document
-
-
Welcome
to the largest Apple community on Lemmy. This is the place where we talk about everything Apple, from iOS to the exciting upcoming Apple Vision Pro. Feel free to join the discussion!
Rules:
- No NSFW Content
- No Hate Speech or Personal Attacks
- No Ads / Spamming
Self promotion is only allowed in the pinned monthly thread
Communities of Interest:
Apple Hardware
Apple TV
Apple Watch
iPad
iPhone
Mac
Vintage AppleApple Software
iOS
iPadOS
macOS
tvOS
watchOS
Shortcuts
XcodeCommunity banner courtesy of u/Antsomnia.
-
A place for conversation about cocktails, ingredients, home mixology, the bar industry or liquor industry, glassware - this is not an exhaustive list. If you think it’s in some way related to cocktails it’s probably fine.
If you post something you didn’t create give credit whenever possible.
Pictures and recipes are encouraged when posting a drink as a standalone post. Example of an ideal drink post:
We love garnishes.
Remember the code of conduct, keep it nice. In terms of cocktails- specific etiquette that might be different from other communities:
Mentioning your blog, insta, website, book or bar is allowed, yes. For now at least, we do allow self-promotion. If it gets out of hand this might change.
A good post with a drink you don’t like is still a good post! Try not to conflate the drink and the post or poster. If someone has a relevant title, gorgeous photo and clearly formatted recipe of what you consider a truly terrible drink, a comment is more appropriate than a downvote.
On that topic: Polite critique/reviews of drinks (or posts, images, etc.) is allowed here. Encouraged , even. It’s a good tool for improving your drinks and content. Really, just be nice.
-
Post your wild Marketplace finds
-
Post your comics here. Single or multi boxed comics.
Please mark nsfw when appropriate.
Same rules as primary server, no hate.
Please warn others if there may be triggers.
Please mark if the comic is yours either in the title or description
obvious ai images will be removed, please include a source to prevent this
-
People tweeting stuff. We allow tweets from anyone.
RULES:
- Mark NSFW content.
- No doxxing people.
- Must be a pic of the tweet or similar. No direct links to the tweet.
- No bullying or international politcs
- Be excellent to each other.
- Provide an archived link to the tweet (or similar) being shown if it’s a major figure or a politician. Archive.is the best way.
-
This is the lemmy community of Monero (XMR), a secure, private, untraceable currency that is open-source and freely available to all.
Wallets
Android (Cake Wallet) / (Monero.com)
iOS (Cake Wallet) / (Monero.com)
Instance tags for discoverability:
Monero, XMR, crypto, cryptocurrency
-
A community for news and discussion about the hardware side of technology. Questions and support posts are also welcome, so long as they are relevant to hardware and interesting technologies therein.
Rules
1. English onlyTitle and associated content has to be in English.
2. Use original linkPost URL should be the original link to the article (even if paywalled) and archived copies left in the body. It allows avoiding duplicate posts when cross-posting.
3. Respectful communicationAll communication has to be respectful of differing opinions, viewpoints, and experiences.
4. InclusivityEveryone is welcome here regardless of age, body size, visible or invisible disability, ethnicity, sex characteristics, gender identity and expression, education, socio-economic status, nationality, personal appearance, race, caste, color, religion, or sexual identity and orientation.
5. Ad hominem attacksAny kind of personal attacks are expressly forbidden. If you can’t argue your position without attacking a person’s character, you already lost the argument.
6. Off-topic tangents
Stay on topic. Keep it relevant.
-
Feddit UK Community for Red Dwarf - (The cult BBC Sci-Fi comedy series)
-
Our favourite hack frauds.
Be nice. All instance rules apply.
Rules:
- Be respectful. Everyone should feel welcome here.
- No bigotry - including racism, sexism, ableism, homophobia, transphobia, or xenophobia.
- No Ads / Spamming.
- No pornography.
Règles :
- Soyez respectueux. Tout le monde doit se sentir le bienvenu ici.
- Pas de bigoterie - y compris le racisme, le sexisme, le capacitisme, l’homophobie, la transphobie ou la xénophobie.
- Pas de publicités / Pas de spam.
- Pas de pornographie.
-
News from civil commercial and noncommercial aviation, videos, discussions, and more.
Basic rules
1. English onlyTitle and associated content has to be in English.
2. No posts about military aviationAvoid any and all posts related to military aviation.
3. No meme postsNo meme posts. Those should go to !aviationmemes@lemm.ee.
4. Instance rules applyAll lemmy.zip instance rules listed in the sidebar will be enforced.
If someone is interested in moderating this community, message @brikox@lemmy.zip.
-
Discussion of climate, how it is changing, activism around that, the politics, and the energy systems change we need in order to stabilize things.
As a starting point, the burning of fossil fuels, and to a lesser extent deforestation and release of methane are responsible for the warming in recent decades:
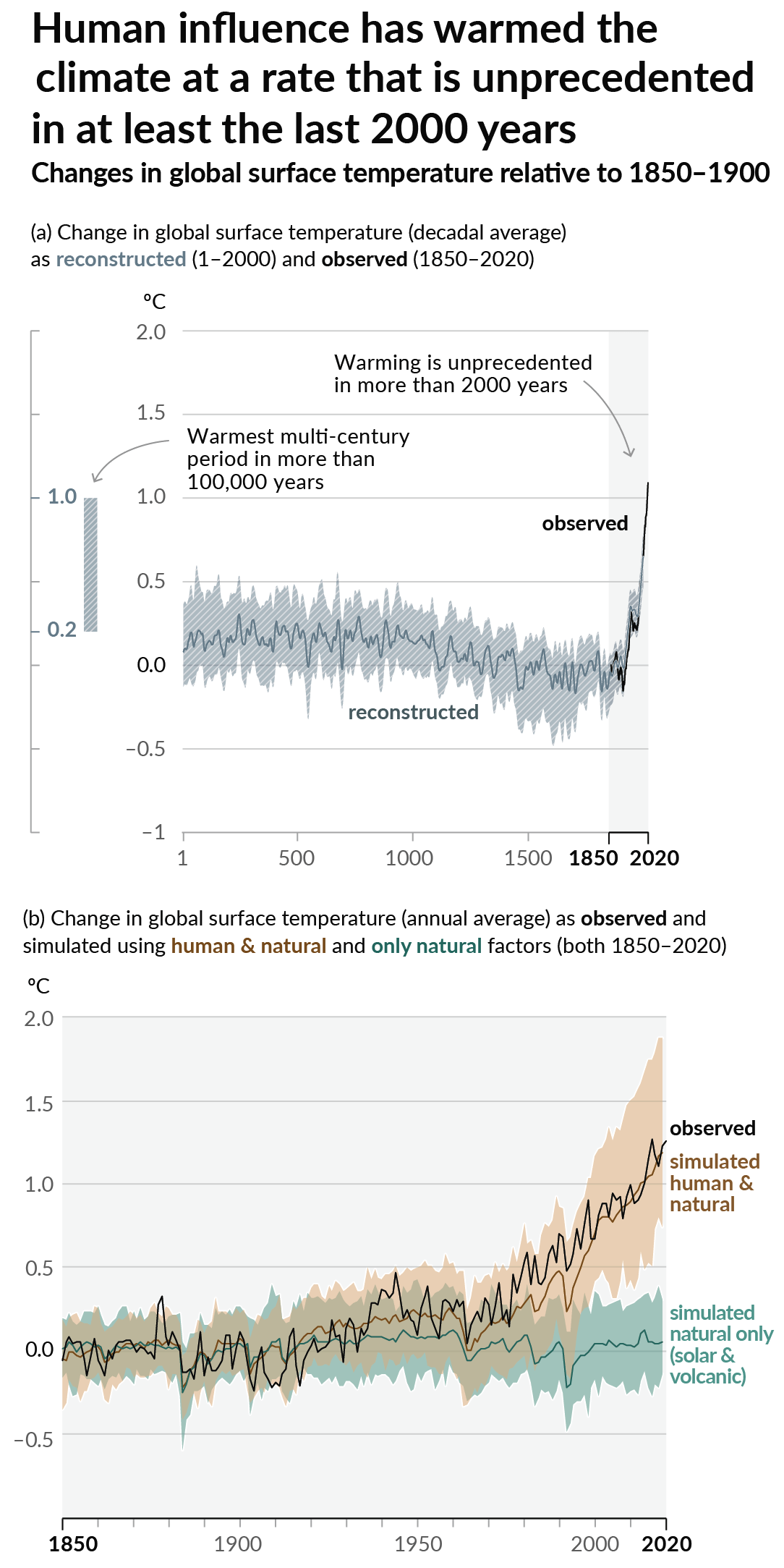
How much each change to the atmosphere has warmed the world:
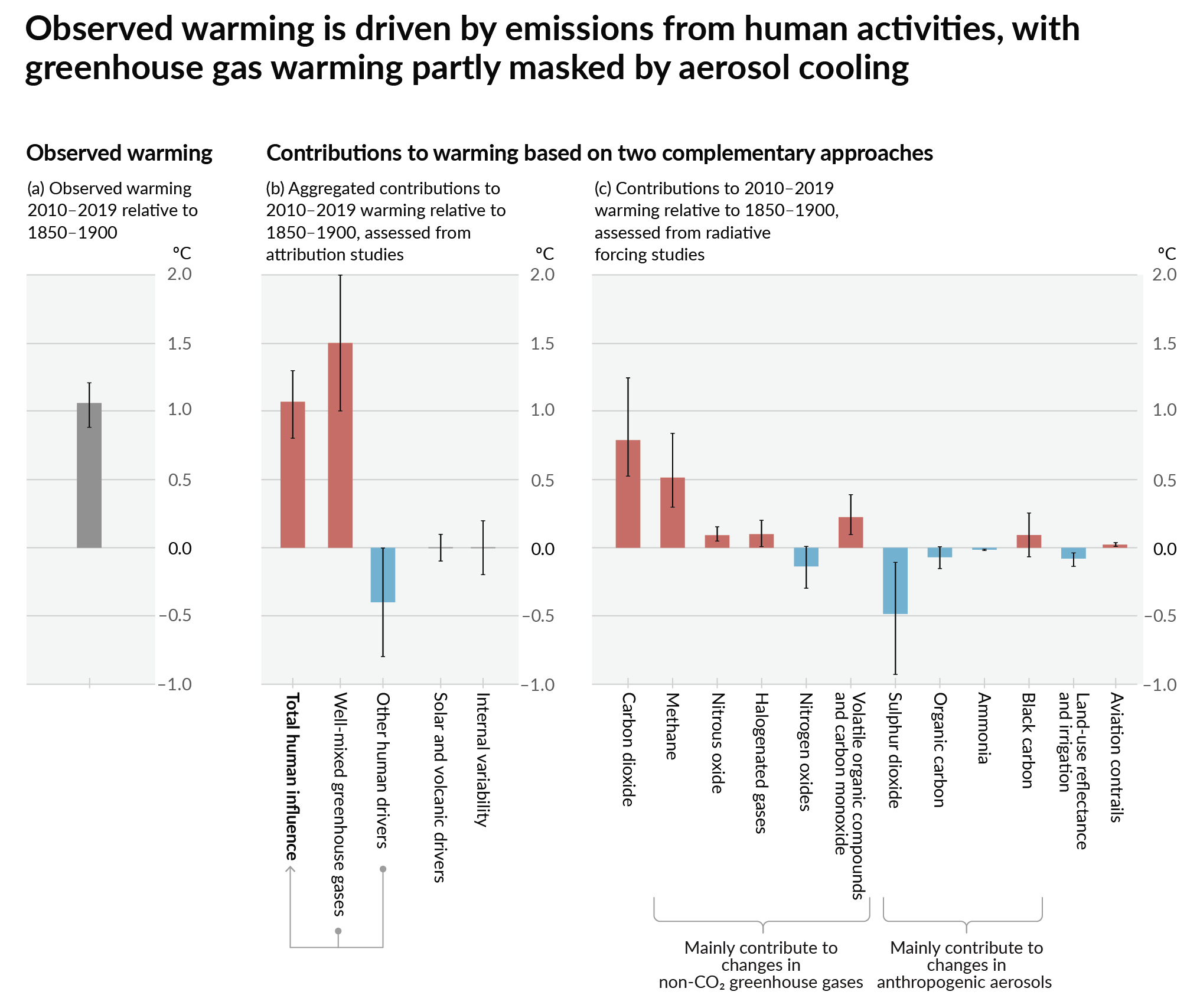
Recommended actions to cut greenhouse gas emissions in the near future:
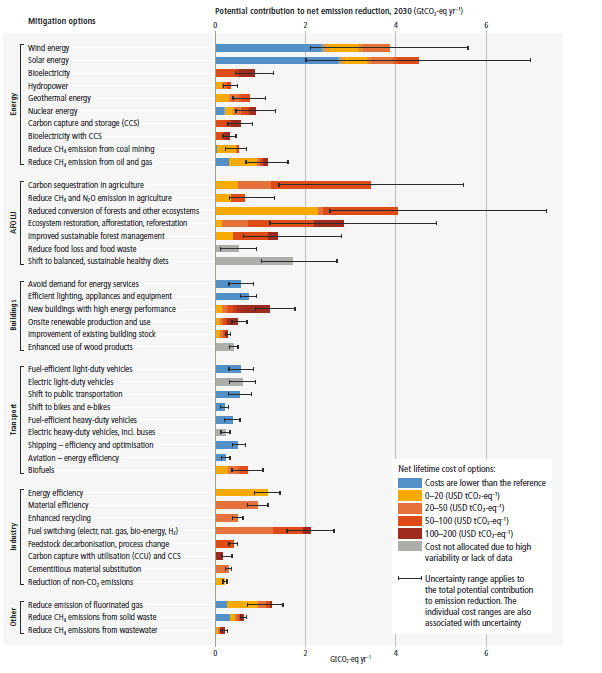
Anti-science, inactivism, and unsupported conspiracy theories are not ok here.
-
People tooting stuff. We allow toots from anyone and are platform agnostic (Mastodon, BlueSky, Twitter, Tumblr, FaceBook, Whatever)
-
A place to post memes & images that won’t absolutely obliterate your mental health! Memes must not stray into hopelessness and be generally positive or neutral.
I made this with my kid in mind, so that they can have a good, safe place to look at memes, just made to make folks laugh and smile!
Only goofs & silliness. (:
- no NSFW. ever.
- no sexually suggestive material
- swearing is fine, but please don’t go overboard.
- no sad or depressing content
- no politics or politically-motivated content – this include comments.
- no outrage content or bait
- no AI-generated images. Understandably, some may slip through the cracks, but assume no malicious intent.
- no AI accusations. Are you unsure? Leave it be. Is it obvious it’s AI? Please report it.
- No spamming of personal links. You can credit an author, but not spam or advertise.
-
“Laugh-a-Palooza: Unleash Your Inner Chuckle!”
Rules
Read Full Rules Here!
Rule 1: Keep it light-hearted. This community is dedicated to humor and laughter, so let’s keep the tone light and positive.
Rule 2: Respectful Engagement. Keep it civil!
Rule 3: No spamming! AI slop will be considered spam at the discretion of moderators
Rule 4: No explicit or NSFW content.
Rule 5: Stay on topic. Keep your posts relevant to humor-related topics.
Rule 6: Moderators Discretion. The moderators retain the right to remove any content, ban users/bots if deemed necessary.
Please report any violation of rules!
Warning: Strict compliance with all the rules is imperative. Failure to read and adhere to them will not be tolerated. Violations may result in immediate removal of your content and a permanent ban from the community.
We retain the discretion to modify the rules as we deem necessary.
-
Lemmy Community for economy, business, politics, stocks, bonds, product releases, IPOs, advice, news, investment, videos, predictions, government, money, politics, debate, current trends and more.
-
A community devoted to one of the most fascinating, mischievous, adorable critters on our planet. Whether you want to share cute and funny photos and videos of these furry creatures, learn more about their behavior and habitats, or find out how to help and protect them, this is the place for you. Join us and discover the amazing world of squirrels!
-
A community for Saskatchewan
Related communities:
Other provincial communities:
- !alberta@lemmy.ca
- !britishcolumbia@lemmy.ca
- !manitoba@lemmy.ca
- !newbrunswick@lemmy.ca
- !newfoundland@lemmy.ca
- Northwest Territories (pending)
- !nova_scotia_general@lemmy.ca
- Nunavut (pending)
- !ontario@lemmy.ca
- !pei@lemmy.ca
- Quebec (pending)
- Yukon (pending)
Image Credits:
-
!relationshipmemes@lemmyis.fun is the place for relationship memes. Whether you’re loved up or single, showing off or sulking, all your relationship memes are welcome here where it’s actually all quite wholesome. We actually think the more sickly-romantic the better here 😂 Have fun all!
A meme as defined by this community is an image that is designed to make a point or be relatable.
For more adult themed memes: !nsfwmemes@lemmynsfw.com
-
A community dedicated to sharing high quality images of space and the cosmos
Rules:
Include some context in the title (such as the name of the astronomical object or location where it was photographed) Only images, pictures, collages, albums, and gifs are allowed. Please link images from high quality sources ([Imgur](imgur.com), [NASA](https://apod.nasa.gov/apod/archivepix.html), [ESA](https://www.esa.int/ESA_Multimedia/Images), [Flickr](Flickr.com), [500px ](500px.com), etc.) Videos, interactive images/websites, memes, and articles are not allowed Only submit images related to space. This may include pictures of space, artwork of space, photoshopped images of space, simulations, artist’s depictions, satellite images of Earth, or other related images Be civil to one another
-
Rules
- Posts must begin with “TIL”.
- Posts must be about a specific fact. No “TIL about [ducks].”
-
Ask Lemmy community on sh.itjust.works. Ask us anything you feel like asking, just make sure it’s respectful of others and follows the instance rules.
-
Dunking on Liberals from a leftist, anti-capitalist perspective.
“The white liberal differs from the white conservative only in one way: the liberal is more deceitful than the conservative. The liberal is more hypocritical than the conservative. Both want power, but the white liberal is the one who has perfected the art of posing as the Negro’s friend and benefactor; and by winning the friendship, allegiance, and support of the Negro, the white liberal is able to use the Negro as a pawn or tool in this political “football game” that is constantly raging between the white liberals and white conservatives.” — Malcolm X
Rules:
- No liberals. Shitty centrist drivel will earn you a ban.
- No bigotry of any kind.
- Bernie Sanders is still a liberal.
We allow posts about liberal behavior even off fedi, shitposts, and rational, leftist discussion.
Sister community:
!tankiejerk@anarchist.nexusInspired by !tankiejerk@lemmy.world
-
Be cool to each other. We’ll welcome most occult themes, it’s okay if you stray from witchcraft a bit.
No advertising. No trolling. No hate. Violaters will be removed unceremoniously.
We love art credits when possible.
-
For stuff that’s neat. Neat article? Neat video? Neat pic of a bug you saw? All good. Neat meme? Ehhh… take it to the meme subs.
Rules
- Don’t be an asshole. If you’re reading a comment you’re about to make and think “Hmm… this sounds like the kind of comment an asshole would make” then do not make that comment. Yes, even if the other person “started it”. The report button is your friend.
-
Tips & trips to be more productive and get stuff done!
-
This is the place to be on the interweb when Reddit irreversibly becomes a meme itself and implodes
If you are existing mods from r/dankmemes, you should be mod here too, kindly DM me on either platform
The many rules inherited from
- Be nice, don’t be not nice
- No Bigotry or Bullying
- Don’t be a dick!
- Censor any and all personal information from posts and comments
- No spam, outside links, or videos.
- No Metabaiting
- No brigading
- Keep it dank!
- Mark NSFW and spoilers appropriately
- NO REEEEEEE-POSTS!
- No shitposting
- Format your meme correctly. No posts where the title is the meme caption!
- No agenda posting!
- Don’t be a critic
- Karma threshold? What’s that?
-
BBC News - News Front Page
-
A community for all things to do with Europe as well as the EU/EEA.
-
-
Welcome to /c/funny, a place for all your humorous and amusing content.
Looking for mods! Send an application to Stamets!
Our Rules:
-
Keep it civil. We’re all people here. Be respectful to one another.
-
No sexism, racism, homophobia, transphobia or any other flavor of bigotry. I should not need to explain this one.
-
Try not to repost anything posted within the past month. Beyond that, go for it. Not everyone is on every site all the time.
Other Communities:
-
/c/TenForward@lemmy.world - Star Trek chat, memes and shitposts
-
/c/Memes@lemmy.world - General memes
-
-
Welcome to the best community for shitposting.
This community is ad free: No watermarks allowed, don’t spam.
Not Allowed: - Link posts; - Photos of short texts.
-
For news articles which seem so much like satire that you’re surprised they’re not from The Onion.
Rules
- Headlines must exactly match the articles’.
- Posts must be genuine news articles, not satire, opinion, or tabloid pieces.
- News must be current.
- Popular political, religious, or social views are not Oniony, no matter how ridiculous you may think them.
-
No foul language - i.e. French 🤮
Obviously satire, dozy wankers
-
-
Oooooooooooooooooooooooooooooooooooooooooooo…
-
Share shirts that go hard.
Community Rules
1) Be nice and have fun.Site-wide Lemmy.world terms of service apply here. Please familiarize yourself with them.
- No racism, xenophobia, sexualism, supremacism, sexualization of minors, rape content, or gore.
AI generated content of any kind is not allowed in this community; as decided by the community of July 2025
- No Mockup Shirts - We want to see the actual shirt worn in real life, not just a depiction.
- No Advertising - This applies to someone else or yourself.
- No Spamming - Please refrain from sharing the same thing over and over again, and/or posting new content more than three times a day.
Thank you.
-
Welcome to /c/UpliftingNews (rules), a dedicated space where optimism and positivity converge to bring you the most heartening and inspiring stories from around the world. We strive to curate and share content that lights up your day, invigorates your spirit, and inspires you to spread positivity in your own way. This is a sanctuary for those seeking a break from the incessant negativity and rage (e.g. schadenfreude) often found in today’s news cycle. From acts of everyday kindness to large-scale philanthropic efforts, from individual achievements to community triumphs, we bring you news—in text form or otherwise—that gives hope, fosters empathy, and strengthens the belief in humanity’s capacity for good, from a quality outlet that does not publish bad copies of copies of copies.
Here in /c/UpliftingNews, we uphold the values of respect, empathy, and inclusivity, fostering a supportive and vibrant community. We encourage you to share your positive news, comment, engage in uplifting conversations, and find solace in the goodness that exists around us. We are more than a news-sharing platform; we are a community built on the power of positivity and the collective desire for a more hopeful world. Remember, your small acts of kindness can be someone else’s big ray of hope. Be part of the positivity revolution; share, uplift, inspire!
-
Latest and most exciting developments in AI. Info on both local and commercial models.
No bigotry - including racism, sexism, ableism, homophobia, transphobia, or xenophobia.
Be respectful, especially when disagreeing. Don’t be a dick. Don’t be a baby. No name-calling. Everyone should feel welcome here.
No serial downvoting just because you think all AI is “slop.”
-
A community for some of the worst movies ever made
-
A community for USPS employees, their friends and interested bystanders. This is not endorsed by USPS, nor is it able to answer for USPS. The employees are not here to help with your package questions, tracking issues, etc. If you have general questions about postal delivery, working for USPS, etc, feel free to chime in.
-
Links from posts on Lemmy, for which there is a misleading thumbnail.
Friends from other places:
How to make a post?
- For the link, use the original image or website link from the other post
- For the title, describe what the subject of the thumbnail appears to be, and don’t describe the full-size image in any way.
- Add a link to the original post in the post body or comments (to help people discover new content and communities)
Detailed Description, based off the description from the subreddit:
A place to share links that, when posted to Lemmy, generate a thumbnail that misleads people into seeing something entirely different than what the full-size image ends up being. This almost always occurs in an unexpected fashion, where shrinking down an image to thumbnail-size suddenly creates an illusion one would not have expected.
Note that your particular front-end or app may cause the illusion to be different!
Rules
Please use the report button on posts that don’t fit the theme!
-
Only post images where the Lemmy thumbnail creates a unique optical illusion, causing the subject in the thumbnail to appear to be something totally different from the subject in the full-size image. Some content will be better off posted to different communities.
-
No images that are essentially what you say they are.
-
No images that are intentionally set up to mislead or intentionally designed to look like your post title. This includes AI generated illusions.
-
Do not post images that are screenshots or that have superimposed text.
-
No NSFW posts for now
-
-
We’re trying to reduce the numbers of hours a person has to work.
-
We talk about the end of paid work being mandatory for survival.
Partnerships:
- Matrix/Element chatroom
- Discord (channel: #antiwork)
- IRC: #antiwork on IRCNow.org (i.e., connect to ircs://irc.ircnow.org and
/join #antiwork) - Your facebook group link here
- Your x link here
- lemmy.ca/c/antiwork
-
General discussions about “science” itself
Be sure to also check out these other Fediverse science communities:
-
travel
-
-
Twitter or X or whatever you wanna call it lol
-
-
This is a friendly community for everyone who wants to share their art with the world! Everyone is welcomed 🎨
Please visit lemmy.world/c/artmarket as well! This is a community for artists to post their portfolios and announce availability to take commissions, as well as get visibility for Ko-fi, Patreon, and other funding for art activities.
Rules
AI Art: While we appreciate AI generated art, there are more appropriate communities to post that type of art to. Please keep posts to non-AI generated art only. This rule includes AI art that was then manually manipulated (e.g. drawing on top of something generated by AI).
NSFW Policy: Nudity and suggestive content has always been a part of art, but it may be something that some users don’t wish to see or cannot view in certain circumstances (e.g. at work). If your work contains nudity or suggestive content, please mark it as NSFW. Work that contains nudity or suggestive content that is not marked as NSFW will be taken down. As long as the NSFW tag is used, we welcome nude or suggestive subject matter. If you aren’t sure if your work is NSFW or not, just ask yourself, “Could I look at this at a typical office job and not get into trouble?” If you’re still not sure after that, you should probably mark it as NSFW just to be on the safe side.
Spam: Please do not spam this community. Self promotion is fine if you just want people to be aware of your work, but blatant attempts at spam will result in the past being removed and possibly a ban. If you aren’t sure if what you are posting is spam, please contact the moderator first.
Conduct: Be nice, and don’t be a jerk. Constructive criticism is OK, but don’t be mean. Encouragement is always welcomed.
-
Dog bite severity varies by the breed of dog, and studies have found that pit bull–type dogs have both a high rate of reported bites and a high rate of severe injuries, compared to other non–pit bull–type dogs.
Pit bull–type dogs are extensively used in the United States for dogfighting, a practice that has continued despite being outlawed. Several nations and jurisdictions restrict the ownership of pit bull–type dogs through breed-specific legislation.
The sole goal for this comm is to ban pit bulls from every jurisdiction and to treat the remaining ones with respect while every caretaker follows the required safety precautions to keep everyone safe. Dog breeds with documented health issues should also be prevented from being forcibly bred into this world.
Rules:
-
Keep it civil.
-
No advocating for violence.
-
No pit bull advocate gaslighting. Though good faith debates are allowed.
Links:
Dogsbite.org is routinely slandered by the pro-pit lobby, but the site is informative and its data collection procedures are transparent and well-documented.
Pit Nutter Bingo Cliched excuses and problematic arguments pit nutters use.
-
-
A Community for people to create posts with GIFs, MP4s or WEBPs - anything that’s animated and reasonably short.
Images can be often be hosted directly on Lemmy, or on external sites such as imgur.com or catbox.moe.
-
-
This community is abouty the U.S. Green Party and its global counterparts.
It will be a space to explore Green policies, news, and updates on environmental, social, and economic issues worldwide.
-
The latest news and developments on Firefox and Mozilla, a global non-profit that strives to promote openness, innovation and opportunity on the web.
You can subscribe to this community from any Kbin or Lemmy instance:
Related
- Firefox Customs: !FirefoxCSS
- Thunderbird: !Thunderbird
Rules
While we are not an official Mozilla community, we have adopted the Mozilla Community Participation Guidelines as far as it can be applied to a bin.
Rules
-
Always be civil and respectful
Don't be toxic, hostile, or a troll, especially towards Mozilla employees. This includes gratuitous use of profanity. -
Don't be a bigot
No form of bigotry will be tolerated. -
Don't post security compromising suggestions
If you do, include an obvious and clear warning. -
Don't post conspiracy theories
Especially ones about nefarious intentions or funding. If you're concerned: Ask. Please don’t fuel conspiracy thinking here. Don’t try to spread FUD, especially against reliable privacy-enhancing software. Extraordinary claims require extraordinary evidence. Show credible sources. -
Don't accuse others of shilling
Send honest concerns to the moderators and/or admins, and we will investigate. -
Do not remove your help posts after they receive replies
Half the point of asking questions in a public sub is so that everyone can benefit from the answers—which is impossible if you go deleting everything behind yourself once you've gotten yours.
-
For exceptionally interesting content
Rules:
- Posts must be interesting
- Posts must be based in reality
- No hateful content
- No harmful content
- Beauty is in the eye of the beholder
-
A community to chronical lemmy.world’s descent into complete Zionism.
Share modlogs of bans, share evidence of their wrongdoing, or just share memes about Zionist apologia relevant to Lemmy.world.
This is an anarchist community, Zionist or capitalist apologia will not be tolerated in any way.
-
Naming and shaming all “recurring spending models” where a one-time fee (or none at all) would be appropriate and logical.
Expect use of strong language.
Follow the basic rules of lemmy.world and common sense, and try to have fun if possible.
No flamewars or attacking other users, unless they’re spineless corporate shills.
Note that not all subscriptions are awful. Supporting your favorite
camgirlcreator or Lemmy server on Patreon is fine. An airbag with subscription is irl Idiocracy-level dystopian bullshit.New community rule: Shilling for cunty corporations, their subscriptions and other anti-customer practices may result in a 1-day ban. It’s so you can think about what it’s like when someone can randomly decide what you can and can’t use, based on some arbitrary rules. Oh what, you didn’t read this fine print? You should read what you’re agreeing to.
==========
Some other groovy communities for those who wish to own their products, their data and their life:
Some other useful links:
Louis Rossman’s YouTube channel
Look at content hosted at Big Tech without most of the nonsense:
-
News and information from Europe 🇪🇺
(Current banner: La Mancha, Spain. Feel free to post submissions for banner images.)
Rules (2024-08-30)
- This is an English-language community. Comments should be in English. Posts can link to non-English news sources when providing a full-text translation in the post description. Automated translations are fine, as long as they don’t overly distort the content.
- No links to misinformation or commercial advertising. When you post outdated/historic articles, add the year of publication to the post title. Infographics must include a source and a year of creation; if possible, also provide a link to the source.
- Be kind to each other, and argue in good faith. Don’t post direct insults nor disrespectful and condescending comments. Don’t troll nor incite hatred. Don’t look for novel argumentation strategies at Wikipedia’s List of fallacies.
- No bigotry, sexism, racism, antisemitism, islamophobia, dehumanization of minorities, or glorification of National Socialism. We follow German law; don’t question the statehood of Israel.
- Be the signal, not the noise: Strive to post insightful comments. Add “/s” when you’re being sarcastic (and don’t use it to break rule no. 3).
- If you link to paywalled information, please provide also a link to a freely available archived version. Alternatively, try to find a different source.
- Light-hearted content, memes, and posts about your European everyday belong in other communities.
- Don’t evade bans. If we notice ban evasion, that will result in a permanent ban for all the accounts we can associate with you.
- No posts linking to speculative reporting about ongoing events with unclear backgrounds. Please wait at least 12 hours. (E.g., do not post breathless reporting on an ongoing terror attack.)
- Always provide context with posts: Don’t post uncontextualized images or videos, and don’t start discussions without giving some context first.
(This list may get expanded as necessary.)
Posts that link to the following sources will be removed
- on any topic: Al Mayadeen, brusselssignal:eu, citjourno:com, europesays:com, Breitbart, Daily Caller, Fox, GB News, geo-trends:eu, news-pravda:com, OAN, RT, sociable:co, any AI slop sites (when in doubt please look for a credible imprint/about page), change:org (for privacy reasons), archive:is,ph,today (their JS DDoS websites)
- on Middle-East topics: Al Jazeera
- on Hungary: Euronews
Unless they’re the only sources, please also avoid The Sun, Daily Mail, any “thinktank” type organization, and non-Lemmy social media (incl. Substack). Don’t link to Twitter directly, instead use xcancel.com. For Reddit, use old:reddit:com
(Lists may get expanded as necessary.)
Ban lengths, etc.
We will use some leeway to decide whether to remove a comment.
If need be, there are also bans: 3 days for lighter offenses, 7 or 14 days for bigger offenses, and permanent bans for people who don’t show any willingness to participate productively. If we think the ban reason is obvious, we may not specifically write to you.
If you want to protest a removal or ban, feel free to write privately to the admin that applied the rule (check modlog first to find who was it.)
-
nostalgia noun nos·tal·gia nä-ˈstal-jə nə-, also nȯ-, nō-; nə-ˈstäl- 1: a wistful or excessively sentimental yearning for return to or of some past period or irrecoverable condition also : something that evokes nostalgia
Rules for Nostalgia Lemmy Community
1. Respectful Nostalgia Share nostalgic content and memories respectfully. Avoid offensive or insensitive references that may be hurtful to others.
2. Relevant Nostalgia Posts should focus on nostalgic content, including memories, media, and cultural references from the past. Stay on topic to preserve the nostalgic theme of the community.
3. Source Verification If you share nostalgic media or content, provide accurate sources or background information when possible.
4. No Spamming Avoid excessive posting of similar nostalgic topics to keep content diverse and engaging for all members.
5. Positive Discussions Encourage positive discussions and interactions related to nostalgic topics. Respect different viewpoints and memories shared by community members.
6. Quality Content Strive to post high-quality content that sparks nostalgia and meaningful conversations among members.
7. Moderation Guidelines
-
Respectful Behavior Treat fellow members with kindness and respect. Harassment or disrespectful behavior will not be tolerated.
-
Appropriate Content Only Ensure all content aligns with the nostalgic theme and community guidelines. Inappropriate or offensive material will be removed.
-
Engagement and Participation Engage actively with posts and discussions. Constructive feedback and contributions enrich the community experience.
By adhering to these rules and guidelines, we can create a welcoming and enjoyable space to relive nostalgic moments together. If you have any questions or suggestions, feel free to reach out to the moderators. Thank you for sharing your nostalgia responsibly!
-
-
Share your New York Times gift articles links here.
Rules:
- Only post New York Times gift article links.
Info:
- The NYT Open Team. (2021-06-23). “A New Way to Share New York Times Stories”. open.nytimes.com.
- “Gift Articles for New York Times Subscribers”. (n.d.). help.nytimes.com.
Tip:
- Google “unlocked_article_code” and limit search results to the past week.
- Mastodon: Use control-F or ⌘-F to search this page. (ref)
-
Chess Puzzles
Let’s enjoy chess puzzles in this community !
Resources
-
For issues concerning:
- Public Health
- Global Health
- Health Systems & Policy
- Environmental Health
- Epidemiology
- etc.
🩺 This community has a broader scope so please feel free to discuss. When it may not be clear, leave a comment talking about why something is important.
Related Communities
- Medical Community Hub
- Medicine
- Medicine Canada
- Premed
- Premed Canada
- Public Health (📍)
See the pinned post in the Medical Community Hub for links and descriptions. link (!medicine@lemmy.world)
Rules
Given the inherent intersection that these topics have with politics, we encourage thoughtful discussions while also adhering to the mander.xyz instance guidelines.
Try to focus on the scientific aspects and refrain from making overly partisan or inflammatory content
Our aim is to foster a respectful environment where we can delve into the scientific foundations of these topics. Thank you!
-
Share tech news or talk about events in the technology field.
This community is an attempt to spread communities out more from lemmy.world and lemmy.ml, so its less centralized and using the advantages of the fediverse.
-
-
Learn about budgeting, saving, getting out of debt, credit, investing, and retirement planning. Join our community, read the PF Wiki, and get on top of your finances!
Note: This community is not region centric, so if you are posting anything specific to a certain region, kindly specify that in the title (something like [USA], [EU], [AUS] etc.)
-
Discussions of Paranoia, how to apply it in a digital ecosystem (Security, Privacy, Tools, Applications, Questions)
Rules
- Be nice
- Stay on topic
- Don’t farm rage
- Be respectful of others
-
-
A community for those that would like to get away from Google.
Here you may post anything related to DeGoogling, why we should do it or good software alternatives!
Rules
-
Be respectful even in disagreement
-
No advertising unless it is very relevent and justified. Do not do this excessively.
-
No low value posts / memes. We or you need to learn, or discuss something.
Related communities
!privacyguides@lemmy.one !privacy@lemmy.ml !privatelife@lemmy.ml !linuxphones@lemmy.ml !fossdroid@social.fossware.space !fdroid@lemmy.ml
-
-
Are you tired of going into controversial threads and having people not discuss things, circlejerking, or using emotional responses in place of logic? Us too.
Welcome to Actual Discussion!
DO:
- Be civil. This doesn’t mean you shouldn’t challenge people, just don’t be a dick.
- Upvote interesting or well-articulated points, even if you may not agree.
- Be prepared to back up any claims you make with an unbiased source.
- Be willing to be wrong and append your initial post to show a changed view.
- Admit when you are incorrect or spoke poorly. Upvote when you see others correct themselves or change their mind.
- Feel free to be a “Devil’s Advocate”. You do not have to believe either side of an issue in order to generate solid points.
- Discuss hot-button issues.
- Add humour, and be creative! Dry writing isn’t super fun to read or discuss.
DO NOT:
- Call people names or label people. We fight ideas, not people here.
- Ask for sources, and then not respond to the person providing them.
- Mindlessly downvote people you disagree with. We only downvote people that do not add to the discussion.
- Be a bot, spam, or engage in self-promotion.
- Duplicate posts from within the last month unless new information is surfaced on the topic.
- Strawman.
- Expect that personal experience or morals are a substitute for proof.
- Exaggerate. Not everyone slightly to the right of you is a Nazi, and not everyone left of you is a Tankie.
- Copy an entire article in your post body. It’s just messy. Link to it, summarize, and add your thoughts.
For more casual conversation instead of competitive ranked conversation, try: !casualconversation@piefed.social
-
About
Community for asking and answering any question related to the life, the people or anything related to the USA. Non-US people are welcome to provide their perspective! Please keep in mind:
- !politicaldiscussion@lemmy.world or !uspolitics@lemmy.world - politics in our daily lives is inescapable, but please post overtly political things there rather than here
- !flippanarchy@lemmy.dbzer0.com - similarly things with the goal of overt agitation have their place, which is there rather than here
Rules
- Be nice or gtfo
- Discussions of overt political or agitation nature belong elsewhere
- Follow the rules of discuss.online
Sister communities
- !askuk@feddit.uk
- !casualuk@feddit.uk
- !casualconversation@lemm.ee
- !yurop@lemm.ee
- !esp@lemm.ee
Related communities
- !asklemmy@lemmy.world
- !asklemmy@sh.itjust.works
- !nostupidquestions@lemmy.world
- !showerthoughts@lemmy.world
- !uspolitics@lemmy.world
- !politics@piefed.social
-
You can ask questions about the Lemmy.nz instance here.
This community also serves as our Meta community, with posts about updates to the Lemmy software on Lemmy.nz or other things relevant to Lemmy.nz users and not relevant to other instances.
-
The world we live in isn’t just dystopic, it isn’t just stupid, trying to describe all the ways it sucks just makes for a really boring story.
-
So I tied a Tamagotchi to my belt, which was the style at the time
Are you a tech enthusiast who also kind-of hates current tech trends? This community is a place to share your gripes with modern technologies, tech-bro culture, “AI the everything”, etc.
Tech-rant memes, articles, or just rant/horror stories: all are welcome.
Related Communities
- !fuck_ai@lemmy.world
- !tech_memes@lemmy.world
-
This is a community for designs specifically crafted to make the experience worse for the user. This can be due to greed, apathy, laziness or just downright scumbaggery.
-
General trans community.
Rules:
-
Follow all blahaj.zone rules
-
All posts must be trans-related. Other queer-related posts go to c/lgbtq.
-
Don’t post negative, depressing news articles about trans issues unless there is a call to action or a way to help.
Resources:
Best resource: github.com/cvyl/awesome-transgender Site with links to resources for just about anything.
Trevor Project: crisis mental health services for LGBTQ people, lots of helpful information and resources: www.thetrevorproject.org
The Gender Dysphoria Bible: useful info on various aspects of gender dysphoria: genderdysphoria.fyi/en
StainedGlassWoman: Various useful essays on trans topics: stainedglasswoman.substack.com
Trans resources: trans-resources.info
[USA] Resources for trans people in the South: southernequality.org/resources/transinthesouth/#p…
[USA] Report discrimination: action.aclu.org/…/report-lgbtqhiv-discrimination
[USA] Keep track on trans legislation and news: www.erininthemorning.com
[GERMANY] Bundesverband Trans: Find medical trans resources: bundesverband-trans.de/…/leitfaden-fuer-behandlun…
[GERMANY] Trans DB: Insurance information (may be outdated): transdb.de
[GERMANY] Deutsche Gesellschaft für Transidentität und Intersexualität: They have contact information for their advice centers and some general information for trans and intersex people. They also do activism: dgti.org
*this is a work in progress, and these resources are courtesy of users like you! if you have a resource that helped you out in your trans journey, comment below in the pinned post and I’ll add here to pass it on
-
-
A place to discuss positive changes that can make work more equitable, and to vent about current practices. We are NOT against work; we just want the fruits of our labor to be recognized better.
Our Philosophies:
- All workers must be paid a living wage for their labor.
- Income inequality is the main cause of lower living standards.
- Workers must join together and fight back for what is rightfully theirs.
- We must not be divided and conquered. Workers gain the most when they focus on unifying issues.
Our Goals
- Higher wages for underpaid workers.
- Better worker representation, including but not limited to unions.
- Better and fewer working hours.
- Stimulating a massive wave of worker organizing in the United States and beyond.
- Organizing and supporting political causes and campaigns that put workers first.
-
A place to share interesting articles from Wikipedia.
Rules:
- Only links to Wikipedia permitted
- Please stick to the format "Article Title (other descriptive text/editorialization)"
- Tick the NSFW box for submissions with inappropriate thumbnails
- On Casual Tuesdays, we allow submissions from wikis other than Wikipedia.
Recommended:
- Use the search box to see if someone has previously submitted an article. Some apps will also notify you if you are resubmitting an article previously shared on Lemmy.
-
Not too short, not too long. Videos to last through your meal.
Rules:
- Submissions must link directly to a video between 5 minutes and 1 hour long.
- Use a duration in your title such as [9:27].
- Be mindful that some people will be watching this while eating. No ‘gross’ content, no NSFL, racism, bigotry, etc.
- Use a title that is descriptive of the actual video.
- Be respectful of other submitters and commenters. Personal attacks, hate speech, bigotry, etc will not be tolerated.
-
For when you need a laugh!
The definition of a “meme” here is intentionally pretty loose. Images, screenshots, and the like are welcome!
But, keep it lighthearted and/or within our server’s ideals.
Posts and comments that are hateful, trolling, inciting, and/or overly negative will be removed at the moderators’ discretion.
Please follow all slrpnk.net rules and community guidelines
Have fun!
-
Wildland fire, wildlands management, forest resilience, and firefighting
-
-
A community to discuss the impacts of climate change on our communities, and to share knowledge an experiences to help those of us that wish to move to mitigate the effects of said climate changes on our future.
-
don’t start no shit
won’t be no shit
-
-
A community for GrapheneOS related questions and discussion.
-
Welcome to Science Facts Community, a place for rare discoveries, space, ancient mysteries, natural wonders, and mind-blowing scientific realities.
Share fascinating science facts, shocking discoveries, and credible posts that spark curiosity about our universe.
Rules:
• Be kind and respectful
• Post with a source/article
-

A community for memes about anime, manga, games or any kind of media about yuri (girls love).
Rules:
- Content must be yuri-related (obviously).
- Cite the source in either the post or in the comments.
- No sexualization of lolis.
- Remember to tag NSFW content.
- If you’re posting a spoiler, say so in the title of the post.
- Try to avoid reposts.
- No homophobia, biphobia, bi erasure, transphobia or any kind of bigotry.
- Be nice to each other, discussions are welcome but keep them civil.
- It’s not mandatory, but please consider including alt-text for accessibility.
Related communities:
-
For making memes about Dune.
-
Memes fun
-
A community for discussion of anything related to television, streaming, movies and cinema.
-
News about Delta Air Lines and their partners, Medallion Program and more.
Not affiliated with Delta Air Lines
-

News and discussions about celebrities, whether they be actors, musicians, social media influences, politicians, or anyone else of reasonable renown, as well as other cultural issues.
Rules:
-
No hate speech, personal attacks, harassment, doxxing, bullying, etc. are all strictly forbidden.
-
Posts must directly relate to Pop Culture in some form. Memes are acceptable if they are not excessive. Moderators have discretion and will work with community members to determine when such content becomes excessive.
-
AI-generated articles, pictures, and videos are prohibited. This does not preclude posts about AI, so long as it is about pop culture.

-
-
A community to share Pizzacake comics
Do not criticize or praise these comics, in fact please talk about other subjects.
-
A generalist Sci-Fi meme community.
The Memiverse:
!90s_memes@quokk.au
!y2k_memes@quokk.au
!philosophymemes@quokk.au
-
The space to discuss Solarpunk itself and Solarpunk related stuff that doesn’t fit elsewhere.
Join our chat: Movim or XMPP client.
-
For fans of Costco
-
Everything about energy production and storage.
Related communities:
-
Welcome!
We strive for high-quality standards on the latest world events.
The basis of these standards comes from the MBFC, which uses an aggregate of methodologies, including the IFCN and World Freedom Indices, to rate the Bias and Factual Reporting of News.
Does your post fit the standards? Check this thread!
Rules:
Rule 1: No Further Gaza/Israel war posts
Rule 2: No US internal news/US politics
Rule 3: Editorials, opinions, analysis, blogs, gifs, memes, etc non-serious news sources
Rule 4: Non-English articles require a translation in the post or comments (mark the title with the source language eg. [FR] for French)
Rule 5: Petitions, advocacy, surveys
Rule 6: All-caps titles
Rule 7: Old news (≥ 1-Month-old) articles
Rule 8: Unlabeled NSFW images/videos
Rule 9: URL shorteners
- The general rules of the sh.itjust.works instance apply!
Thank you.
-
Imaginary art
Rules
-
Titles should be in the format “[Title]” by [Artist]. Posting the year is optional.
-
Please include the image source in the body of the post.
-
No AI art.
-
No screenshots from movies, tv shows, or games. Fanart or concept art from movies/shows/games is allowed.
-
Please mark posts as NSFW if necessary, such as for gore and nudity. Pornography is not allowed.
Imaginary directory: !lemmydirectory@lemmy.dbzer0.com
-
-
Welcome to Enshittification
A community for everyone who misspelt it as enshitification.
“I the onceler felt sad as I watched them all go, but business is business and business must grow, regardless of crummies in tummies you know.”
This is your space to document the decay, demise, and destruction of the tech world as we know it. Share stories, articles, and firsthand experiences that capture the ongoing decline of once-celebrated platforms, services, and companies in the late stage capitalist landscape.
From monopolistic corporate shifts to anti-user updates and the relentless pursuit of profit over quality—if it’s broken, bloated, or just plain bad, it belongs here. We’re here to spotlight the moves that make the tech world worse, one piece of enshittification at a time.
For some more positive takes
!disenshittify@lemmy.cafe !deshittification@thebrainbin.orgGuidelines
🔹 Stay on Topic: Only post content about the decline of tech products, platforms, or companies.
🔹 Quality Content: Give some context when posting links or articles to drive quality discussions.
🔹 Respectful Discussion: Critique companies, crappy tech, and capital, not community members.
🔹 Positive Monday: The first Monday of every month is reserved for positive content only that shows enshittification isn’t inevitable.Join us to expose the changes that ruin the things we once loved and to discuss what comes next in a tech world gone wrong.
-
WorldNews but without all the arbitrary rules
-
Lifting up Chicago activists through community building, mutual aid, and solidarity in the fight against fascism.
-
A community for discussion and democratic decision making in the Divisions by zero.
Anyone with voting rights can open a governance thread and initiate a vote or a discussion. There’s no special keywords you must be aware of before you open a thread, but there are some. here’s the governance thread manual.
Answers
-
Ahoy, me buckos! Welcome to Bikini Bottom Twitter! Your digital reef for the latest salty gossip and treasure tales! And while you’re at it, be sure to drop by the Krusty Krab for a delicious Krabby Patty so I can get yer mon- err I mean, 'cause they’re the best treat under the sea!
Rule 1 - This is Bikini Bottom Twitter, all posts should be Spongebob related in “(Old-School) Twitter-like” form
Rule 2 - Political posts, as long as it follows rule 1, will be permitted, so long as you behave yourselves.
Bikini Bottom Municipal Code §33-07: Anti-Tankie Ordinance Residents are prohibited from circulating tankie ideology or other authoritarian propaganda on Bikini Bottom Twitter. Offenders will be permanently banned from BPT by the BBPD faster than Plankton is ejected from The Krusty Krab.
Rule 3 - Please no reposts within the last couple days, at least
Rule 4 - All posts should be at least above a “Squirdward-krusty-krab-shift” level of effort
Rule 5 - Be chill, be a Patrick not a squidward.
-
Anything related to aircraft, airplanes, aviation and flying. Helicopters & rotorcraft, airships, balloons, paragliders, winged suits and anything that sustains you in the air is acceptable to post here.
-
Blacklisted Sites
List inspired by other community rules.
- Al Jazeera;
- NBC;
- CNBC;
- Substack;
- Tom’s Hardware;
- ZDNet;
- TechSpot;
- Ars Technica;
- Vox Media outlets(including Axios, due to new changes related to trackers on their website);
- Engadget;
- TechCrunch;
- Gizmodo;
- Futurism;
- PCWorld;
- ComputerWorld;
- Mashable;
- Hackaday;
- WCCFTECH;
- Neowin;
- Jacobin;
- Yahoo;
- Freethink;
- Big Think;
- Newsweek.
Technology news, blogs and articles.
Forbidden:
- Paywalled content.
- Older than 1 month articles;
- External video links(non native videos);
- Article talking about article, research or new.(Always use original articles).
-
Overview:
Electric Vehicles are a key part of our tomorrow and how we get there. If we can get all the fossil fuel vehicles off our roads, out of our seas and out of our skies, we’ll have a much better environment. This community is where we discuss the various different vehicles and news stories regarding electric transportation.
Related communities:
- !automotive@discuss.tchncs.de
- !avs@futurology.today
- !byd@lemmy.world
- !ebike@lemm.ee
- !energy@slrpnk.net
- !geely@lemmy.world
- !micromobility@lemmy.world
- !polestar@lemmy.ca
- !rivian@lemmy.zip
- !teslamotors@lemmy.zip
- !xiaomi@lemdro.id
-
General community for news/discussion in the UK.
Less serious posts should go in !casualuk@feddit.uk or !andfinally@feddit.uk
More serious politics should go in !uk_politics@feddit.uk.Try not to spam the same link to multiple feddit.uk communities.
Pick the most appropriate, and put it there.Posts should be related to UK-centric news, and should be either a link to a reputable source, or a text post on this community.
Opinion pieces are also allowed, provided they are not misleading/misrepresented/drivel, and have proper sources.
If you think “reputable news source” needs some definition, by all means start a meta thread.
Posts should be manually submitted, not by bot. Link titles should not be editorialised.
Disappointing comments will generally be left to fester in ratio, outright horrible comments will be removed.
Message the mods if you feel something really should be removed, or if a user seems to have a pattern of awful comments.
-
RULES:
-
Post material that is related to ICE. Could also be about surveillance that aids ICE, how to avoid ICE, etc.
-
Be respectful towards each other. Don’t make anything personal.
-
-
To discuss how to grow and manage communities / magazines on Lemmy, Mbin, Piefed and Sublinks
Resources:
- lemmy-federate.com to federate your community to a lot of instances
- !fedibridge@lemmy.dbzer0.com to organize overall fediverse growth
- !reddit@lemmy.world to keep tabs on where new users might come from :)
- !newcommunities@lemmy.world
- !communitypromo@lemmy.ca
- lemvotes.org
Megathreads:
- How (and when) to consolidate communities? (A guide)
- Where to request inactive or unmoderated communities? (A list)
Rules:
- Be respectful
- No bigotry
-
Grasweeti - Portmanteau of sweet and graffiti
A community to share pictures of cute graffiti, stickers, wheatpastes and more. Be careful to not dox yourself and if you can, please provide an image description (here are some tips for doing that).
-
A hub for discovering and sharing privacy-respecting, open-source, and self-hosted digital tools that improve productivity, creativity, and digital independence.
-
For owls that are superb.

Please scroll down to read our community rules.
US Wild Animal Rescue Database: Animal Help Now
International Wildlife Rescues: RescueShelter.com
Australia Rescue Help: WIRES
Germany-Austria-Switzerland-Italy Wild Bird Rescue: wildvogelhilfe.org
If you find an injured owl:
Note your exact location so the owl can be released back where it came from. Contact a licensed wildlife rehabilitation specialist to get correct advice and immediate assistance.
Minimize stress for the owl. If you can catch it, toss a towel or sweater over it and get it in a cardboard box or pet carrier. It should have room to be comfortable but not so much it can panic and injure itself. If you can’t catch it, keep people and animals away until help can come.
Do not give food or water! If you feed them the wrong thing or give them water improperly, you can accidentally kill them. It can also cause problems if they require anesthesia once help arrives, complicating procedures and costing valuable time.
If it is a baby owl, and it looks safe and uninjured, leave it be. Time on the ground is part of their growing up. They can fly to some extent and climb trees. If animals or people are nearby, put it up on a branch so it’s safe. If it’s injured, follow the above advice.
For more detailed help, see the OwlPages Rescue page.
Community Rules:
Posts must be about owls. Especially appreciated are photographs (not AI) and scientific content, but artwork, articles, news stories, personal experiences and more are welcome too.
Be kind. If a post or comment bothers you, or strikes you as offensive in any way, please report it and moderators will take appropriate action.
AI is discouraged. If you feel strongly that the community would benefit from a post that involves AI you may submit it, but it might be removed if the moderators feel that it is low-effort or irrelevant.
Also visit our twinned community for wholesome content:
!wholesome@reddthat.com
-
The Elder Scrolls (TES) is an award-winning RPG series by Bethesda Softworks set in the vast world of Nirn.
RULES:
-
This is an all-purpose community. Almost anything relating to The Elder Scrolls is welcome, be it in-depth lore discussions, memes, or casual chats.
-
Off-topic discussion in parent posts (Included but not limited to irl politics, religion, real world issues) is banned. You can discuss it to a light level in the comments, if it’s in relation to the games.
-
Racism, sexism, homophobia, transphobia, xenophobia, and ableism is not allowed, and will result in a ban.
-
Explicitly NSFW content is prohibited.
-
AI-generated content is prohibited.
-
-
For all things related to the City of Tacoma.
-
Rules •1. No Doxxing •2. No TikTok reposts •3. No Harassing •4. Post Gore at your own discretion, Depends if its funny or just gore to be an edgelord.
-
Welcome to politcal memes!
These are our rules:
1) Be civilJokes are okay, but don’t intentionally harass or disturb any member of our community. Sexism, racism and bigotry are not allowed. Good faith argumentation only. No posts discouraging people to vote or shaming people for voting.
2) No misinformationDon’t post any intentional misinformation. When asked by mods, provide sources for any claims you make.
3) Posts should be memesRandom pictures do not qualify as memes. Relevance to politics is required.
4) No bots, spam or self-promotionFollow instance rules, ask for your bot to be allowed on this community.
5) No AI generated content.Content posted must not be created by AI with the intent to mimic the style of existing images
-
All posts need to have the same title: me_irl it is allowed to use an emoji instead of the underscore _
-
Mr. Lovenstein
An unoffical Lemmy community dedicated to Mr. Lovenstein comics!
Share and discuss your favorite Mr. Lovenstein comics.
Rules
- Only post images of Mr. Lovenstein comics.
-
A community where you can ask questions about what hardware supports GNU/Linux, how to get things working, places to buy from (i.e. they support GNU/Linux) and so on.
Quick rules:
- Be nice to each other.
- Report toxic people.
EXTERNAL RESOURCES
- Linux on Laptops[↗]
- OpenPrinting Database[↗]
- RHEL Compatibility Database[↗]
- Wifi Adapter Compatibility Database[↗]
- FSF Hardware Database[↗]
GNU/LINUX VENDORS
- Entroware[↗] [UK/Eire]
- Juno Computers[↗] [UK/USA]
- Ministry of Freedom[↗] [UK]
- System76[↗] [USA]
- ThinkPenguin[↗] [USA]
- Tuxedo Computers[↗] [Germany]
OTHER VENDORS
- Dell[↗] (certain lines) [Global]
- Lenovo[↗] (X and T lines) [Global]
- Raspberry Foundation via various vendors
Webcasts
-
Banned? DM Wmill to appeal.
No anti-nautilism posts. See: Eco-fascism Primer
Slop posts go in c/slop. Don’t post low-hanging fruit here.
-
Discussion of the various incarnations on the Traveller RPG by Marc Miller, et al.
-
Kia ora and welcome to !newzealand, a place to share and discuss anything about Aotearoa in general
- For politics , please use !politics@lemmy.nz
- Shitposts, circlejerks, memes, and non-NZ topics belong in !offtopic@lemmy.nz
- If you need help using Lemmy.nz, go to !support@lemmy.nz
- NZ regional and special interest communities
Rules:
FAQ ~ NZ Community List ~ Join Matrix chatroom
Banner image by Bernard Spragg
-
H.P. Lovecraft’s Cthulhu Mythos is a shared universe far larger and more terrifying than that of humanity, where ancient, malevolent beings known as the Great Old Ones slumber in the depths of space or time. After Lovecraft’s death, the Mythos has been expanded and developed by many authors, including August Derleth, Clark Ashton Smith, and Robert E. Howard. These and many other authors have helped to flesh out the Mythos into a rich and complex Dark Universe.
Rules:
-
Please NO “Call of Cthulhu RPG” content. Post them on !callofcthulhu@ttrpg.network
-
PLEASE ONLY MYTHOS-INSPIRED CONTENTS
-
Share stories, books, authors and any other works from the mythos
-
Share reviews, analysis and theories on the lore
-
Share videos, images and contents inspired by the lore
-
Where possible share the link to the authors or the sources
-
Ignore the call in your dreams as long as possible
🐙 For more cosmic horror: !cosmichorror@piefed.social 🐙
💀 For more horror content: !horror@lemmy.ca 💀
🎲 For Call of Cthulhu RPG
!callofcthulhu@ttrpg.network 🎲
📅 New videogame/movie release:
#Horror, #Cosmic Horror, #science fiction,
-
-
Hint:
:q!
Sister communities:* !tech_memes@lemmy.world * !memes@lemmy.world * !lemmyshitpost@lemmy.world * !risa@startrek.website
Community rules (click to expand) :::spoiler 1. Follow the site-wide rules
- Instance-wide TOS: legal.lemmy.world/tos/
- Lemmy code of conduct: join-lemmy.org/docs/code_of_conduct.html ::: :::spoiler 2. Be civil
- Understand the difference between a joke and an insult.
- Do not harrass or attack users for any reason. This includes using blanket terms, like “every user of thing”.
- Don’t get baited into back-and-forth insults. We are not animals.
- Leave remarks of “peasantry” to the PCMR community. If you dislike an OS/service/application, attack the thing you dislike, not the individuals who use it. Some people may not have a choice.
- Bigotry will not be tolerated. :::
- Including Unix and BSD. - Non-Linux content is acceptable as long as it makes a reference to Linux. For example, the poorly made mockery of
sudoin Windows. - No porn, no politics, no trolling or ragebaiting. - Don’t come looking for advice, this is not the right community.:::spoiler 4. No recent reposts
- Everybody uses Arch btw, can’t quit Vim, <loves/tolerates/hates> systemd, and wants to interject for a moment. You can stop now. ::: :::spoiler 5. 🇬🇧 Language/язык/Sprache
- This is primarily an English-speaking community. 🇬🇧🇦🇺🇺🇸
- Comments written in other languages are allowed.
- The substance of a post should be comprehensible for people who only speak English.
- Titles and post bodies written in other languages will be allowed, but only as long as the above rule is observed. ::: :::spoiler 6. (NEW!) Regarding public figures We all have our opinions, and certain public figures can be divisive. Keep in mind that this is a community for memes and light-hearted fun, not for airing grievances or leveling accusations.
- Keep discussions polite and free of disparagement.
- We are never in possession of all of the facts. Defamatory comments will not be tolerated.
- Discussions that get too heated will be locked and offending comments removed. :::
Please report posts and comments that break these rules!
Important: never execute code or follow advice that you don’t understand or can’t verify, especially here. The word of the day is credibility. This is a meme community – even the most helpful comments might just be shitposts that can damage your system. Be aware, be smart, don’t remove France.
-
LANCER is the tabletop role playing game of mech combat created by Tom Parkinson-Morgan and Miguel Lopez.
Each player takes the role of an upcoming mech pilot in the tumultuous year of 5016u. The game features robust mech customization and deadly tactical combat.
-
Community Guide
Archive Today will help you look at paywalled content the way search engines see it.
Statement of Purpose
- This is a support and conversation community for people who don’t believe in gods.
- Superstition hucksters have no reason to subscribe or post here at all.
- If you are looking to debate or proselytize, options will be linked lower in the sidebar.
Acceptable
- Honest questions or conversations.
- Discussions on parenting or advice.
- Struggles, frustrations, coming out.
- Atheist memes. We can have fun!
- News headlines relevant to atheism.
Unacceptable
Depending on severity, you might be warned before adverse action is taken.
- Anything against site rules.
- Illegal and/or NSFW material.
- Troll posts and comments. There will be no attempt to explain what that means.
- Leading questions, agenda pushing, or disingenuous attempts to bait members.
- Personal attacks or flaming.
Inadvisable
- Self promotion or upvote farming.
- Excessive shitposting or off-topic discussion.
Application of warnings or bans will be subject to moderator discretion. Feel free to appeal. If changes to the guidelines are necessary, they will be adjusted.
If you vocally harass or discriminate against any individual member, you will be removed.
Likewise, if you are a member, sympathizer or a resemblant of a group that is known to largely hate, mock, discriminate against, and/or want to take lives of any other group of people, and you were provably vocal about your hate, then you you will be banned on sight.
Provable means able to provide proof to the moderation, and, if necessary, to the community.
~ /c/nostupidquestions
If you want your space listed in this sidebar and it is especially relevant to the atheist or skeptic communities, PM DancingPickle and we’ll have a look!
Connect with Atheists
- Matrix: #atheism:envs.net
Help and Support Links
- Freedom From Religion Foundation
- The Secular Therapy Project
- Secular Students Alliance
- Black Nonbelievers
- The Clergy Project
- Atheist Alliance International
- Sunday Assembly
- Atheist Ireland
- Atheism UK
- Atheists United
Streaming Media
This is mostly YouTube at the moment. Podcasts and similar media - especially on federated platforms - may also feature here.
- Atheist Debates - Matt Dillahunty
- Rationality Rules
- Friendly Atheist
- Making Sense with Sam Harris
- Cosmic Skeptic
- Genetically Modified Skeptic
- Street Epistemology
- Armored Skeptic
- NonStampCollector
Orgs, Blogs, Zines
- Center for Inquiry
- American Atheists
- Humanists International
- Atheist Republic
- The Brights
- The Angry Atheist
- History for Atheists
- Rationalist International
- Atheist Revolution
- Debunking Christianity
- Godless Mom
- Atheist Freethinkers
Mainstream
Bibliography
Start here…
…proceed here.
- God is Not Great (Hitchens)
- The God Delusion (Dawkins)
- The End of Faith (Harris)
- Why I Am Not a Christian (Russell)
- Letter to a Christian Nation (Harris)
Proselytize Religion
From Reddit
As a community with an interest in providing the best resources to its members, the following wiki links are provided as historical reference until we can establish our own.
-
Starfleet HQ
The Federations source for all Star Trek news, updates, and discussion.
Rule 1 — Be Civil, Not KlingonEngage respectfully with fellow crew members.
Rule 2 — Stay On Topic
- No harassment, brigading, or trolling
- No bigotry (racism, sexism, transphobia, etc.)
- Disagreeing is fine, but personal attacks are not
Posts should be related to Star Trek: news, updates, official announcements, or meaningful discussion.
Rule 3 — No Prohibited Content
- Off-topic content may be removed
- Memes should be quarantined under a level 5 containment field to !Risa@lemmy.dbzer0.com
Some things are not allowed aboard the ship.
Rule 4 — Gatekeeping Is Not Starfleet
- No spam or scams
- No illegal content
- No porn or sexually explicit material
- NSFW content must be properly tagged
You can have your opinions on what counts as “real” Star Trek, but forcing them on others is not allowed.
- Everyone’s perspective is valid, TOS purists and Lower Decks fans alike
- Keep debates about canon and quality friendly and inclusive
If you see a post breaking the rules, report it so the moderators can handle it. If you’d like to be a mod, shoot Stamets a message.
-
Welcome to the community for independent journalism, a place to post and engage with diverse, free news media from around the world.
The rundown:
-
Posts should link to a current* article from a credible, English, independent news source. If there’s a paywall, please put the official link in the URL box and add an archive link in the text body of your post. Blogs, editorials, listicles and reports are welcome.
-
Post title should be the article headline or best fit. Add this tag if an account is needed for access: [sign-in required.]
-
No misinformation. Provide sources when making substantial or potentially destructive claims.
-
Be civil. Be respectful. Be cool. Instance rules apply.
-
Tag NSFW and apply content warnings at your discretion.
*Independent journalism is generally free from government and corporate interests and is not controlled by a major media conglomerate. “Independence” is a gradient, so use your best judgement when posting.
*Current depends on whether new, publicly available information has been released since the article has last been updated. When in doubt please add the published date to the title in a tag [like this.]
For a less serious news community, check out: !wildfeed@sh.itjust.works
Canadian-based independent news: !indy_news_canada@sh.itjust.works
All communities were created with the goal of increasing media literacy and media pluralism.
Some of the independent news sources posted here:
Australia
Canada
Germany
India
Philippines
Russia
meduza.io/en (based in Latvia)
South Africa
U.S.A.
Global
-
-
-

For all things Tolkien, Lord of The Rings (LotR), and The Hobbit across all media. Speak friend and enter.
Rules:
- No abusive language
- No buying, selling or advertising
- Be civil
- No politics
- No discussions about race
- No bots
- No memes or AI-generated content
- Don’t criticize others for their opinions
- If you found the image on the web, it is encouraged to put the direct link to the image in the ‘Link’ field when creating a post, instead of uploading the image to Lemmy. Direct links usually end in .jpg, .png, etc.
- No unrelated posts
- No spoilers in title, mark spoilers
- Let people like what they like
- Follow all Lemmy.world rules
Please report any rule violations.
-
We are a community that posts tweets and have a good laugh. We allow tweets from anyone. We welcome anyone who follows the rules to participate here.
-
A community about dogs.
Breeds, tips and tricks about training and behaviour, news affecting dog owners, canine photography, dog-related art and any questions related to dog ownership.
Rules
- Posts must be related to dogs or dog ownership and must not be void of content.
- This is a neutral space. No bigotry or personal attacks. Criticism should be polite and constructive.
- No automated content. This includes AI generated imagery, post body, articles, comments or automated accounts.
- No advertising or self-promotion.
- Illegal or unethical practices are frowned upon, and any comments or posts suggesting them will be removed. This includes, but is not limited to, backyard breeding, ear and tail cropping, fake service animals, negative reinforcement, alpha/pack/dominance theory, and eugenics.
- No judging or attacking community members who care for dogs with cropped ears, docked tails, or those from puppy mills or questionable sources. While we discourage these practices (per Rule 5), all dogs deserve loving homes and compassionate care regardless of their background or physical alterations.
- No breed discrimination, all breeds welcome. Our stance matches the ASPCA’s official stance and is not up for debate.
- Citing your sources when making a claim is encouraged. Misinformation will be removed.
-
Just look at some of these kids, how can they be so dumb? Like what, you seriously can’t hula hoop? Jesus christ. And babies know literally nothing. God damn kids are so dumb.
The rules:
1. Your post must depict a kid doing something stupid. No simple accidents, unless the accident was caused by stupidity. No memes, either. A story (e.g., a tweet) is okay.
2. Re-posts will be removed at mod discretion.
3. Posts have to be funny or cringey. If the kid really gets hurt, it’s no fun.
4. Sitewide rules apply. Basically, (a) don’t be a dick; (b) use the NSFW tag; © no spam; (d) don’t attack people; and (e) don’t abuse the report button.
Partnered communities:
-
-
Welcome to /c/Battlestations
A community for sharing your computer, gaming or work setups as well as discussion about anything related to such setups.
- Posts should include a photo of a computer setup of some kind or be a discussion of computer setups.
- Posts or comments that are homophobic, transphobic, racist, sexist, ableist, or advocating violence will be removed.
- Be civil: disagreements happen, but that doesn’t provide the right to personally insult others.
- Spam, self promotion, trolling, and bots are not allowed
-
c/space Rules
- Submissions must be related to Space
- No sensationalist/ misleading/ unscientific content
- No spam
- No low-effort or meme images
-
A Community for the Cities Skylines game by Colossal Order on Lemmy.
-------------------------------------
About Cities Skylines
Raise a city from the ground up and transform it into a thriving metropolis with the most realistic city builder ever. Push your creativity and problem-solving to build on a scale you’ve never experienced. With deep simulation and a living economy, this is world-building without limits.
-------------------------------------
Community Bookmarks
-------------------------------------
➤ Simple Guidelines
➧1. All content must be related to Cities Skylines
➧2. No spam or reposts. Do not submit more than one of the same post/comment on this community or across multiple communities.
➧3. Be respectful. Harassment, abuse, name calling, and/or threats of any kind is not tolerated here. Any content, whether an image or a comment, that includes any kind of bigoted language or hate speech will be met with a permanent ban.
➧4. Check before posting · Posts about or which ask questions already addressed will be removed.
➧5. No advertisement or self-promotion. Do not use this community to advertise or self-promote. This includes (but is not limited to) websites, articles, blog posts, and brands. We welcome occasional links to your own off-site content like Twitch and YouTube/Invidious.
➧6. No NSFW Posts · Nudity: Obvious, implied or strategically covered · Content that is “sexually explicit”, gore.
➧7. Links · All shared links must be from Paradox/Colossal Order websites/forums, excluding links to Youtube/Invidious videos and trusted news sources (about the games). Latter ones must respect ‘Rule 4’.
➧8. Piracy · Discussion is allowed, sharing links is not (view the rule above).
➧9. Memes · Memes are allowed, but please keep it low or it will be considered as spam.
Read the extensive Guidelines.
Comply with the Lemmy Code of Condute.
➠Feel free to report any content that does not respect these rules.
-------------------------------------
Community Filters
(uses phtn.app)
-
Discussion of table top roleplaying games.
-
Non political memes: !memes@sopuli.xyz
-
Community of SimpleX Chat users – managed by the team.
SimpleX Chat is the first chat platform that is 100% private by design – it has no user identifiers of any kind and no access to your connections graph – it’s a more private design than any alternative we know of.
Please ask any questions and make feature suggestions. Your ideas and criticism are very welcome!
-
A community for sharing your worlds, exploring others’ worlds, and discussing anything relating to the art of worldbuilding.
Related Communities:
Rules:
- Follow Lemmy’s Code of Conduct.
- Remain on-topic. Worldbuilding contains many areas of interest, so, when in doubt, explain how your contribution fits within worldbuilding.
- Give context in the comments of your post. This will help your audience engage with your creation and encourage interaction.
- Tag posts as NSFW if they contain images or discussion of extreme violence or explicit sexuality.
- Advertising should not disrupt the community. Self-promotion of projects related to worldbuilding are fine. However, you must be willing to engage with your audience.
- Love each other. There’s a human on the other side of your screen, so treat them with respect.
-
A place to share business news and insights.
Rules
- Follow lemmy.world rules
- Only post content related to business
- Do not use this community to promote your business
-
Liminal spaces are the subject of an Internet aesthetic portraying empty or abandoned places that appear eerie, forlorn, and often surreal. Liminal spaces are commonly places of transition (pertaining to the concept of liminality) or of nostalgic appeal.
-
Rules:
-
No sympathy with the enemy or its collaborators. Russian and North Korean soldiers are fascists committing a genocide. Remember that.
-
Objective and factual reporting from the battlefield, parliaments, etc. is encouraged, even if it’s about bad news for Ukraine.
-
Insulting Putin and his cronies (Orban, Trump, Musk,…) is absolutely fine but don’t use homophobic or similar language against them. Members of the queer community don’t deserve to be compared to that scum. Also: Putin disciminates against gay people. If you do as well, you’re part of the problem.
-
Don’t insult or use overly harsh language against other commentators.
-
Don’t submit direct links to Twitter/X and Truth Social posts. You may: Post a screenshot + quote, do a full quote and name the author, direct link to a proxy service like xcancel.com, deep link an image embedded in a tweet because Lemmy will cache a copy.
-
Don’t just complain about paywalls. If you encounter one, be a sport and link to an archived version instead. Use Firefox + uBlock Origin with the annoyances filters enabled and filterlists.com/…/bypass-paywalls-clean-filter to avoid encountering many in the first place.
-
-
!britishcolumbia@lemmy.ca
News, highlights and more relating to this great province!
-

Welcome to c/plantid @ Mander.xyz!
AKA What’s this plant?
Notice Board
This community is a work in progress, stay tuned while we build the ID bot and set up shop.
- 2023-06-16: Feel free to resubmit your images if the ID bot is not triggered while we test the bot. If uploading does not work, try uploading on imgur. The URL of the image needs to be placed in the URL of the post.
- 2023-06-15: ID Bot v1.0 is up and working. Ongoing testing. Please ignore the test posts.
About
Whether you’re seeking help with identifying a particular plant or eager to share your own findings, our community is here to offer support and foster a love for exploration. We believe in collaborative and inclusive learning, providing guidance, and celebrating the joy of discovery as we deepen our understanding of the natural world.
Rules
- Don’t throw mud. Be kind and remember the human.
- Keep it rooted (on topic).
- No spam.
The Bot
How to Use:
- Upload your image and place the URL in the URL line of the post. The comments are not set up yet nor is post body.
Tips:
- Isolate a feature of the plant, such as a leaf or a flower, for best ID.
Open Source Code:
Get involved in Citizen Science: Add your photo here to help build a database of plants across the entire planet. This database is used by non-profits, academia, and the sciences to promote biodiversity, learning and rewilding.
Resources
- PlantNet | PlantNet GitHub
- Python Script to batch ID photos locally in a directory.
- Foraging & Wild Foods Map
See the sidebar at !houseplants@mander.xyz for a more detailed list.

Similar Communities
DM us to add yours! :)
General
Gardening
- !balconygardening@slrpnk.net
- !gardening@mander.xyz
- !nativeplantgardening@mander.xyz
- !gardening@lemmy.ml
- !gardening@midwest.social
- !permaculture@lemmy.world
- !tropical_plants@mander.xyz
Species
- !bonsai@tchncs.de
- !succulents@midwest.social
- !mosses@mander.xyz
- !fruit@slrpnk.net
Regional
Science
Sister Communities
Science and Research
Biology and Life Sciences
- !anthropology@mander.xyz
- !biodiversity@mander.xyz
- !palaeoecology@mander.xyz
- !palaeontology@mander.xyz
Plants & Gardening
- !balconygardening@slrpnk.net
- !gardening@mander.xyz
- !houseplants@mander.xyz
- !plantid@mander.xyz
- !plantswap@mander.xyz
Physical Sciences
Humanities and Social Sciences
Memes
-
Welcome
Visit us on Matrix at #geopol:matrix.org
-
This is a no agenda less moderated variation of !climate@slrpnk.net. Moderation power is not abused and mods do not suppress ideas in order to control the narrative.
Obvious spam, uncivil posts and misinfo are not immune to intervention, but on-topic civil posts are certain to not be subject to censorship (unlike the excessive interventalism we see in the other climate community).
-
About Community
c/Cars is the largest automotive enthusiast community on Lemmy and the fediverse. We’re your central hub for vehicle-related discussion, industry news, reviews, projects, DIY guides, advice, stories, and more.
Rules
- Stay respectful to the community, hold civil discussions, even when others hold opinions that may differ from yours.
- This is not an NSFW community, and any such content will not be tolerated.
- Policy, not politics! Policy discussions revolve around the concept; political discussions revolve around the individual, party, association, etc. We only allow POLICY discussions and political discussions should go to c/politics.
- Must be related to cars, anything that does not have connection to cars will be considered spam/irrelevant and is subject to removal.
-
In the attention economy, your time is your most valuable curency - and you are being robbed of it in broad daylight…
or, should I say, screenlight.
It’s not your fault… but it IS within your power to do something about it.
Take your time back.
Take your attention back.
Take your life back.
And then go to TakeOurTimeBack to help others do the same at scale.
-
Overview:
The community dedicated to boycotting the US until they stop fascism, restore full democracy and start following international law.
Americans have a moral obligation to resist Donald Trump and project 2025 at every turn.
America is a flawed democracy currently being ruled by oligarchs. Stop the backslide! Dont let America become the next Hungary.
America needs to challenge the court rulings of citizens united v. fec and shelby county v. holder, protect the media, implement independent district drawing, and the single transferable vote so they don’t end up having people stay home in life-changing elections because they cannot vote for their favourite candidate.
Join 50501.chat to fight back!
Related communities:
Boycott:!buycanadian@lemmy.ca !buyeuropean@feddit.uk !boycott@lemmy.sdf.org !boycottchina@sopuli.xyz
Activism:!antitrumpalliance@lemmy.world !petitions@lemmy.ca !palestine@lemmy.dbzer0.com !protest@lemmy.world !israelicrimes@lemmy.world !patriotsforprogress@lemmy.ca !goodsuniteus@lemmy.ca
-
A girls mix doing this and that, most of them by themselves
-
Lemmy placeholder and fan community for the Endless Thread podcast. Podcast hosts Ben Brock Johnson and Amory Sivertson dig into.untold histories, unsolved mysteries and other wild stories from online communities, collaborating with members of those online communities. Produced by WBUR, Boston’s NPR station.
Not affiliated with Endless Thread or WBUR.
Follow the Lemmy.world Code of Conduct
-
Welcome to the lemmy.world community for Portland, Oregon!
This community has kind of been empty since it was created, I’m hoping to change that!
Unlike “other” Portland communities you may have seen “elsewhere”, I believe in a “warts and all” approach. You are free to take off your Rose tinted glasses and talk about topics that are dragging our city down.
At the same time, sunset pics, snowmageddon, traffic monster, cones, that’s all welcome as well. Let’s collectively keep Portland weird!
2024 is going to be an interesting year politically with all the changes to city government, I will attempt to tag political threads with a [Politics] tag and encourage users to do so as well.
Other than the lemmy.world restrictions on spam, copyrighted material, and adult material (USE that NSFW tag!), there’s only one real way to get in trouble here:
- Don’t attack other users.
It’s OK to go after Teargas Ted, it’s OK to say Rene Gonzales is a fascist, ACAB, BLM, whatever floats your boat (WEFYB).
It’s NOT OK to attack or diminish another user. Feel free to disagree, you can point out the many ways you think they’re wrong, just don’t start throwing perjoratives AT OTHER USERS.
Links to know!
Portland Trailblazers Schedule!
Portland Winterhawks Home Game Schedule!
www.rosequarter.com/events/winterhawks
Portland Timbers Pre-Season Starts in February!
-
This community has been locked, please see the discussion here. The original sidebar contents can be found below:
--- # Rules 1. Any drama must be posted as an observer, you cannot post drama that you are involved with. 2. When posting screenshots of drama, you must obscure the identity of all the participants. 3. The poster must have a credible post and comment history before submitting a piece of history. This is to avoid sock-puppetry and witch hunts. The usual instance-wide rules also apply. --- Chronicle the life and tale of the fediverse (+ matrix) Largely a sublemmy about capturing drama, from fediverse spanning drama to just lemmy drama. Includes lore like how a instance got it's name, how an instance got defederated, how an admin got doxxed, fedihistory etc (New) This sub's intentions is to an archive/newspaper, as in preferably don't get into fights with each other or the ppl featured in the drama Tags: fediverse news, lemmy news, lemmyverse Partners: * [midwest.social/c/Fediverse](https://midwest.social/c/fediverse) * [Sub promo](https://lemmy.ca/c/communitypromo) * [Fedizens](https://lemmy.ca/c/fedizens)
The original community icon is here
-
Are we checking? This is a place to take a p*ss out of motorsports.
F1 is not the only motorsport in the world, so go ahead and post your shitposts about WEC or MotoGP or IndyCar or ralley or Polish Speedway or whatever. Even Formula E, I guess. It needs some love, too.
By the way, F2 > F1.
Rules? What rules? Stop inventing. Just don’t be a douche. Lemmy.world’s sporting conduct applies.
If you experience connectivity issues read catbox.moe/faq.php
-
dank memes
Rules:
-
All posts must be memes and follow a general meme setup.
-
No unedited webcomics.
-
Someone saying something funny or cringe on twitter/tumblr/reddit/etc. is not a meme. Post that stuff in /c/slop
-
Va*sh posting is haram and will be removed.
-
Follow the code of conduct.
-
Tag OC at the end of your title and we’ll probably pin it for a while if we see it.
-
Recent reposts might be removed.
-
No anti-natalism memes. See: Eco-fascism Primer
-
-
Community for the city of Vancouver, BC
-
Don’t trash (talk) the nati’
Welcome to c/cincinnati - a community for Cincinnati, OH
Related Cincinnati communities
General
Sports
-
A community for posting memes relating to linux!
Also check out:
Original icon base courtesy of lewing@isc.tamu.edu and The GIMP
-
This community is for getting help with vehicle or other mechanical problems.
Remember, there are no stupid questions, we want everyone to feel welcome. If you don’t want to answer a question that you think is silly, then just move on and keep it to yourself.
Rules:
- Don’t be a dick
That is all.
-
A place for any post topic you want to talk about in an active conversation with digital neighbors of the threadiverse. Treat this place like your real neighbors that live three or four doors away.
Report anything. All mod actions are harmful, and all posts and comments get the benefit of doubt if at all possible.
-
Hjælp og råd, spørgsmål og svar, how-tos etc. Hvis du gerne vil skifte fra ondsindet tech, så få hjælp her! Alle emner er velkomne.
-
Community Guidelines:
1. memes only please, serious discussion is for other comms
2. memes that glorify states will be removed
3. genAI art in memes is OK, but memes should be marked AI generated (please)
4. no bigotry of any kind
5. if you post angry replies you will get made fun of
6. don’t be liberal scum 💩
7. zionists/nazis will be banned preemptively because they deserve death
8. no fedposting
-
About
Hello fellow Cyanide and Happiness fans!
Cyanide & Happiness (C&H) is a webcomic created by Rob DenBleyker, Kris Wilson, Dave McElfatrick and Matt Melvin. The comic has been running since 2005 and is published on the website explosm.net along with animated shorts in the same style. Matt Melvin left C&H in 2014, and several other people have contributed to the comic and to the animated shorts
Read more: en.wikipedia.org/wiki/Cyanide_%26_Happiness
Hope you enjoy and feel free to contribute to the community with art, media, cool stuff about the authors, tattoos, toys and anything else, as long it’s Cyanide & Happiness related!
History
@MrSebSin@sh.itjust.works started this community and wrote:
About this community and how I post the comics… Many moons ago, I would ask my Dad to save the newspaper for me everyday so I could read my favorite comic strips. Of course these days you can read your favorite comics online instead of a newspaper, but I love the nostalgia of reading the daily comics. Anyway, one of my favorite current comics is Cyanide and Happiness and I will be posting the daily release from their website (explosm.net) and a an extra or two randoms.
Related Communities
Subscribe to all the daily comic communities!
- !BelloBearOfficial@lemmy.world - Bello Bear
- !BloomCounty@sopuli.xyz - Bloom County
- !CalvinAndHobbes@lemmy.world - Calvin and Hobbes
- !CyanideAndHappiness@lemm.ee - Cyanide and Happiness
- !Garfield@lemmy.world - Garfield
- !Moomin@sopuli.xyz - Moomin Valley
- !Oglaf@midwest.social - Oglaf (Very NSFW!)
- !Peanuts@midwest.social - Peanuts
- !pbf@discuss.online - The Perry Bible Fellowship
- !SMBC@midwest.social - SMBC
- !TheFarSide@sh.itjust.works - The Far Side
- !XKCD@lemmy.world - XKCD
Fine Print
All comics posted are freely available online. In no way is the poster claiming ownership, copyright or anything else. This is a not for profit community, we just want to enjoy our comics, thank you.
-
A community to discuss all things about the fallout video game series and it’s lore.
With this community, I want to help with expanding Lemmy’s content while also utilizing other instances. I am new to moderating a community but hope to help bring in discussion about what brought us here to begin with.
We follow the same rules as our instance sopuli.xyz
-
Welcome to /c/houseplants @ Mander.xyz!
In between life, we garden.

About
We’re a warm and informative space for plant enthusiasts to connect, learn, and flourish together. Dive into discussions on care, propagation, and styling, while embracing eco-friendly practices. Join us in nurturing growth and finding serenity through the extraordinary world of houseplants.
Need an ID on your green friends? Check out: !plantid@mander.xyz
Get involved in Citizen Science: Add your photo here to help build a database of plants across the entire planet. This database is used by non-profits, academia, and the sciences to promote biodiversity, learning and rewilding.
Rules
- Don’t throw mud. Be kind and remember the human.
- Keep it rooted (on topic).
- No spam.

Resources
Recommendations
Health
Identification
- PlantNet.org (see also: !plantid@mander.xyz)
- Seek from iNaturalist
Light Information
- GrowLightMeter
- PlantLightDB
- HouseplantJournal (Scroll down.)
Databases
- Catalogue of Life
- Perenual.com
- The Garden.org Plants Database
- Useful Tropical Plants (Interactive Database Version)
- WorldFloraOnline
- USA-NPN
- Tom Clothier’s Garden Walk and Talk
- Plants for a Future
- USDA Datasets
- Permapeople.org
- Temperature Climate Permaculture: Plant Index
- Natural Capital Plant Database
- Colorado Plant Database
- SEINet
- North American Ethnobotany Database
- BCSS Field No. Lookup (collection site IDs for cacti and succulents)
- U Michigan Native Plant Database for Michigan by Region
FOSS Tools
- Common House Plants API
- HappyPlants (Monitoring App)
- PlantGeek (Care Info App)
Similar Communities
DM us to add yours! :)
General
Gardening
- !balconygardening@slrpnk.net
- !gardening@mander.xyz
- !nativeplantgardening@mander.xyz
- !gardening@lemmy.ml
- !gardening@midwest.social
- !permaculture@lemmy.world
- !tropical_plants@mander.xyz
Species
Regional
Science
Sister Communities
Science and Research
Biology and Life Sciences
- !anthropology@mander.xyz
- !biodiversity@mander.xyz
- !palaeoecology@mander.xyz
- !palaeontology@mander.xyz
Plants & Gardening
Physical Sciences
Humanities and Social Sciences
Memes
-
Welcome to c/Fallout, the unofficially official community to discuss the franchise.
Be sure to check out !falloutmods@lemmy.world, moderated by a friend of ours :)
Join us on matrix.to/#/#falloutnewmatrix:matrix.org!
Rules:
-
Keep it civil. Don’t insult other community members in posts or comments, and don’t make posts designed to insult other community members or parts of the fandom with different opinions.
-
Posts must be on-topic.
-
No real life politics. That means no political advocacy, and no real life political discussions vaguely dressed up as on-topic posts. If you want to discuss real life politics, you are free to start your own community.
-
Posts must be coherent.
-
If a post is otherwise allowed but has realistic gore or nudity, please mark it NSFW.
-
Spoilers about newly released official content must be marked as [SPOILERS] with post images blurred and no spoiler information in the thread title. Comments must adhere if the thread OP specified a non-spoiler thread.
PS: Don’t use the fandom! please use fallout.wiki for everything instead.
Banner art by Ivan Kalinin
-
-
Icon base by Delapouite under CC BY 3.0 with modifications to add a gradient
-
The central hub for general practice, clinical updates, and medical news. A curated blend of our community’s voice and global dispatches from the #medicine tag.
-
Ausome Memes
The lighter side of ASD
Rules
Other ND communities
- !adhd@lemmy.dbzer0.com
- !autism@lemmy.dbzer0.com
- !autisticandadhd@lemmy.world
- !neurodivergence@beehaw.org
-
Long-form, in-depth, thought-provoking articles about various topics.
-
Placeholder for any r/CanadaPolitics refugees
Rules
- Keep the original title when submitting an article. You can put your own commentary in the body of the post or in the comment section.
- Has to be relevant to Canadian politics.
Reminder that the rules for lemmy.ca also apply here. See the sidebar on the homepage: lemmy.ca
-
The Heinlein Society
Here to “Pay it Forward” and to discuss the life and works of the Grand Master.
RULES
- Sitewide rules apply.
- No piracy – Please do not recommend piracy here. This means no hints, no links, no suggestions, nothing. If you have found pirated content you wish to report, please go to my profile and send me a message and I’ll take care of it from there.
- As this site is officially for The Heinlein Society and we are a 501(c)(3) non-profit corporation, discussion of current politics is disallowed. Thank you for understanding.
-
Welcome to c/Beavers!
Post your favorite beaver pics and memes here. Show off your beavers!
Our rules for posting and commenting, besides the rules defined here for lemmy.world, are as follows:
- Be respectful and inclusive
Everyone should feel welcome here. Hateful or bigoted language will not be tolerated.
- No illegal or NSFW or NSFL content
Don’t post anything a beaver would not approve of. Yes, we get the double entendre. No, we do not allow those beavers.
- No advertisement or spam
Beavers don’t like spam.
Related Communities
Community Feedback and Moderation
For inquiry on becoming a moderator of this community, please send a message to the current moderators. Any feedback on the community should also be sent to the moderators.
-
A community dedicated to the New England Patriots.
Check out our other sports communities!


North 







East 







South 







West 







-
Fàilte gu Alba!
Mon in tae Scotland!
Welcome to Scotland!
Quick rules:
- dinnae be a cunt
- posts should relate tae Scotland
- one post per topic please
Have at it, and haste ye back
Related communities
-
We are still in this together, but "this" is going to be real different in the very near future. This demands a different kind of "we."
The French Resistance during Nazi occupation played important roles delivering downed Allied airmen back to safety, supplying military intelligence, and acts of sabotage.
The Underground Railroad is estimated to have brought 100,000 freedom seekers to safety between 1810 and 1850.
It's time.
Rules
- Do not gatekeep resistance
- Do not organize specific subversive plans here.
- Do not identify yourself or anyone else here.
- Do brainstorm general ideas about how to support people who need it and stymie the efforts of fascists
- Do share thoughts on how to be personally prepared for subversive action
-
Welcome! This is a community for all those who are interested in protecting their privacy.
Rules
PS: Don’t be a smartass and try to game the system, we’ll know if you’re breaking the rules when we see it!
- Be civil and no prejudice
- Don’t promote big-tech software
- No apathy and defeatism for privacy (i.e. “They already have my data, why bother?”)
- No reposting of news that was already posted
- No crypto, blockchain, NFTs
- No Xitter links (if absolutely necessary, use xcancel)
Related communities:
Some of these are only vaguely related, but great communities.
- !opensource@programming.dev
- !selfhosting@slrpnk.net / !selfhosted@lemmy.world
- !piracy@lemmy.dbzer0.com
- !drm@lemmy.dbzer0.com
-
Welcome to c/linux!
Welcome to our thriving Linux community! Whether you’re a seasoned Linux enthusiast or just starting your journey, we’re excited to have you here. Explore, learn, and collaborate with like-minded individuals who share a passion for open-source software and the endless possibilities it offers. Together, let’s dive into the world of Linux and embrace the power of freedom, customization, and innovation. Enjoy your stay and feel free to join the vibrant discussions that await you!
Rules:
-
Stay on topic: Posts and discussions should be related to Linux, open source software, and related technologies.
-
Be respectful: Treat fellow community members with respect and courtesy.
-
Quality over quantity: Share informative and thought-provoking content.
-
No spam or self-promotion: Avoid excessive self-promotion or spamming.
-
No NSFW adult content
-
Follow general lemmy guidelines.
-
-
What is No Lawns?
A community devoted to alternatives to monoculture lawns, with an emphasis on native plants and conservation. Rain gardens, xeriscaping, strolling gardens, native plants, and much more! (from official Reddit r/NoLawns)
Have questions or don’t know where to begin?
Where can you find the official No Lawns socials?
Rules
- Be Civil
- Don’t dox yourself
- Stay on Topic
- Don’t break instance or Lemmy rules
-
Tripping’ Through Time
A Lemmy community for historic art pieces overhauled into modern memes.
Rules
- Only image uploads allowed
- Only edited, historical images may be shared
- The instance rules of lemmy.ca
-
For PC gaming news and discussion. PCGamingWiki
Rules:
- Be Respectful.
- No Spam or Porn.
- No Advertising.
- No Memes.
- No Tech Support.
- No questions about buying/building computers.
- No game suggestions, friend requests, surveys, or begging.
- No Let’s Plays, streams, highlight reels/montages, random videos or shorts.
- No off-topic posts/comments, within reason.
- Use the original source, no clickbait titles, no duplicates. (Submissions should be from the original source if possible, unless from paywalled or non-english sources. If the title is clickbait or lacks context you may lightly edit the title.)
-
Everything #OpenStreetMap related is welcome: software releases, showing of your work, questions about how to tag something, as long as it has to do with OpenStreetMap or OpenStreetMap-related software.
OpenStreetMap is a map of the world, created by people like you and free to use under an open license.
Join OpenStreetMap and start mapping: www.openstreetmap.org.
There are many communication channels about OSM, many organized around a certain country or region. Discover them on openstreetmap.community
mapcomplete.org is an easy-to-use website to view, edit and add points (such as shops, restaurants and others)
learnosm.org/en/ has a lot of information for beginners too.
-
For debat og nyheder omkring teknologi af alle former.
-
Welcome to BuyFromEU - A community dedicated to supporting European-made goods and services!
Feel free to post, comment and vote, be excellent to each other and follow the rules.
We also invite you to subscribe to:
- !europe@feddit.org
- !europepolitics@feddit.org
- !buyeuropean@feddit.uk
Logo generated with mistral le chat Banner by Christian Lue on unsplash.com
-
Har du gode idéer eller kunne tænke dig at organisere noget? Hørt om noget der sker? Spred rygtet eller find hinanden her.
-
Singapore related posts (any deletion by moderators WILL come with explanation) Moderation will be stepped up as the community grows. Ask Singapore related questions at !asksingapore
-
THE Lemmy community for visual arts. Paintings, sculptures, photography, architecture are all welcome amongst others.
Rules:
- Follow instance rules.
- When possible, mention artist and title.
- AI posts must be tagged as such.
- Original works are absolutely welcome. Oc tag would be appreciated.
- Conversations about the arts are just as welcome.
- Posts must be fine arts and not furry drawings and fan art.
-
/c/TenForward: Your home-away-from-home for all things Star Trek!
Re-route power to the shields, emit a tachyon pulse through the deflector, and post all the nonsense you want. Within reason of course.
~ 1. No bigotry. This is a Star Trek community. Remember that diversity and coexistence are Star Trek values. Any post/comments that are racist, anti-LGBT, or generally "othering" of a group will result in removal/ban.
~ 2. Keep it civil. Disagreements will happen both on lore and preferences. That's okay! Just don't let it make you forget that the person you are talking to is also a person.
~ 3. Use spoiler tags. This applies to any episodes that have dropped within 3 months prior of your posting. After that it's free game.
~ 4. Keep it Trek related. This one is kind of a gimme but keep as on topic as possible.
~ 5. Keep posts to a limit. We all love Star Trek stuff but 3-4 posts in an hour is plenty enough.
~ 6. Try to not repost. Mistakes happen, we get it! But try to not repost anything from within the past 1-2 months.
~ 7. No General AI Art. Posts of simple AI art do not 'inspire jamaharon'
~ 8. No Political Upheaval. Political commentary is allowed, but please keep discussions civil. Read here for our community's expectations.
Fun will now commence.
Sister Communities:
Want your community to be added to the sidebar? Just ask one of our mods!
Creator Resources:
Looking for a Star Trek screencap?
(TrekCore)Looking for the right Star Trek typeface/font for your meme?
(Thank you @kellyaster for putting this together!)
-
A place where the trade community can discuss topics of interest.
Unofficial Discord: discord.gg/qV6MrFXE
-
for discussion of all thing commuting by bike
About
Whether it’s a journey for work, shopping or leisure, maybe even tweaks and hacks to make your commute easier, feel free to share.
Community Guidelines
- Be nice
- No spam/ads
- Follow the rules of the instance we’re hosted on: mastodon.world/about
Partnered Communities
- !micromobility@lemmy.world
Related
- !bicycles@lemmy.ca
- !bicycling@lemmy.world
- !bikewrench@lemmy.world
- !bikepacking@lemmy.world
-
This is a place for beer lovers of all levels to come together and share their love of beer.
-
Big brain tech dude got yet another clueless take over at HackerNews etc? Here’s the place to vent. Orange site, VC foolishness, all welcome.
This is not debate club. Unless it’s amusing debate.
For actually-good tech, you want our NotAwfulTech community
-
Android news for android developers. Everything that happens in android world.
For Android development specific topics please see /c/android_dev
The Android robot is reproduced or modified from work created and shared by Google and used according to terms described in the Creative Commons 3.0 Attribution License
-
A community for oenophiles, vintners, sommeliers and more. For all those who share our love of the nectar of the gods.
-
-
Related Communities !programmerhumor@lemmy.ml !programmer_humor@programming.dev !programmerhumor@kbin.social !programming_horror@programming.dev
Other Programming Communities !programming@beehaw.org !programming@programming.dev !programming@lemmy.ml !programming@kbin.social !learn_programming@programming.dev !functional_programming@programming.dev !embedded_prog@lemmy.ml
-
GIFs and pics of nude celebrities (female only)
-
Big tech and governments are monitoring and recording your eating activities. c/Privacy provides tips and tricks to protect your privacy against global surveillance.
Partners:
- community.nicfab.it/c/privacy
-
Whether it be electronics, automobiles or medical equipment, the manufacturers should not be able to horde “oem” parts, render your stuff useless if you repair it with aftermarket parts, or hide schematics of their products.

Summary video by Marques Brownlee
Great channel covering and advocating right to repair, Lewis Rossman
-
Friendly community for pizza lovers and creators of all levels. Share your creations, recipes or questions!
Logo by catalyststuff on Freepik (freepik.com/…/flying-slice-pizza-cartoon-vector-i…)
-
This is a pro-LGBTQIA+ community.
A community for some conservative points of view. Including general news. We support equal rights here. Just because you don’t like it or it doesn’t align with your views, doesn’t mean it’s not true.
Warning: I have reported, and will keep reporting, extreme posts on Lemmy to the FBI. This is the webpage used to report federal crimes and submit tips regarding violence against elected officials, and domestic terrorism activity. tips.fbi.gov/home
Rule 0: Serial downvoters will be banned.
🍃🌻 Rule 1: Kindly be empathetic and kind to others. Trolling and spamming will not be tolerated.
Rule 2: Keep it Civil - It’s NOT OK to say another USER is a (pejorative) or a paid (pejorative).
Making the community a friendly & supportive place is our goal.
All of us are here for a short lifetime. Let’s have a nice time here and avoid negativity. :)
Please be respectful, even if you don’t agree.
Don’t personally attack people. Don’t call them names.
Be grown-ups.
-
Just crazy ideas!
-
Description
This is a community for sharing those cheesy “dad” jokes that invoke an eye roll or chuckle.
Rules
- Clean jokes only please. If you cannot tell this joke to a 5-year-old and they can understand, you probably shouldn’t post it here. Please post edgier jokes to: !unclejokes@lemmy.world
- Adult topics with which to be cautious or avoided: drugs, sex, death, racism.
- Must post text, image (e.g., meme), or direct link. Do not post external links that cannot be viewed directly from the community (e.g., link to joke website, Facebook, Instagram, etc.)
- Follow Lemmy.World Code of Conduct
-
A safe space to report and discuss the daily abuses of power that occur on the Lemmy.
Naughty List:
- Ye Power Tripping Trippin’ Bastards
-
-
A comm for content and discussions of all things fast food.
Post about coupons, your favorite combo meal, news articles, menu items taken from us far too soon or even memes (as long as it relates to fast food!) 🍕
Fast casual stuff is also welcome here! But politics are not, even if they relate to fast food. This comm is intended to be a light meal, not for discussing the political leaning of a fast food company. If you want to open those kinds of discussions, please checkout !politicaldiscussion@lemmy.world
-
Support and meta community for Beehaw. Ask your questions about the community, technical issues, and other such things here.
A brief FAQ for lurkers and new users can be found here.
Our September 2024 financial update is here.
For a refresher on our philosophy, see also What is Beehaw?, The spirit of the rules, and Beehaw is a Community
This community’s icon was made by Aaron Schneider, under the CC-BY-NC-SA 4.0 license.


-
A community for progressive issues, social justice and LGBT+ causes in media, gaming, entertainment and tech.
Official replacement for Reddit’s r/GamerGhazi
Content should be articles, video essays, podcasts about topics relevant to the forum. No memes, single images or tweets/toots/… please!
Community rules:
Be respectful and civil with each other. Don’t be a jerk. There is a real human being on the other side of your screen. See also the Blahaj.Zone Community Rules
No bigotry of any kind allowed. Making racist, sexist, trans-/homo-/queerphobic, otherwise demeaning and hateful comments is not ok. Disabilities and mental illnesses are not to be used as insults and should not be part of your comment unless speaking of your own or absolutely relevant.
No gatekeeping and being rude to people who don’t agree with you. Leave “gamer” stereotypes out of your comment (e.g. sexless, neck bearded, teenaged, basement-dwelling, etc). Don’t compare people to animals, or otherwise deny their humanity. Even if you think someone is the worst human on the planet, do not wish death or harm upon them.
No “justice porn”. Posts regarding legal action and similar is allowed, but celebrating someone being harmed is not.
Contrarianism for its own sake is unnecessary and not welcome.
No planning operations, no brigading, no doxxing or similar activities allowed.
Absolutely no defense of GamerGate and other right-wing harassment campaigns, no TERFs and transphobia, racism, dismissing of war crimes and praise of fascists. This includes “JAQing off”, intentionally asking leading questions while pretending to be a neutral party. This also applies to other forms of authoritarianism and authoritarian or criminal actions by liberal or leftist governments.
NSFW threads, such as ones discussing erotic art, pornography and sex work, must be tagged as such.
Moderators can take action even if none of the rules above are broken.
-
A community for respectful discussion and memes related to autism acceptance. All neurotypes are welcome.
Community:
Values- Acceptance - Openness - Understanding - Equality - Reciprocity - Mutuality - Love
Rules1) No abusive, derogatory, or offensive post/comments e.g: racism, sexism, religious hatred, homophobia, gatekeeping, trolling. 2) Posts do not need be related to autism, off-topic discussions are allowed. This is a safe space where people with autism can feel comfortable discussing whatever they feel like discussing, as long as it does not violate the standing rules. 3) Your posts must include a text body. It doesn’t have to be long, it just needs to be descriptive. 4) Do not request donations. 5) Be respectful in discussions. 6) Do not post misinformation. 7) Mark NSFW content accordingly. 8) Do not promote Autism Speaks. 9) General Lemmy World rules. 10) No bots. Humans only.
Encouraged1) Open acceptance of all autism levels as a respectable neurotype. 2) Funny memes. 3) Respectful venting. 4) Describe posts of pictures/memes using text in the body for our visually impaired users. 5) Welcoming and accepting attitudes. 6) Questions regarding autism. 7) Questions on confusing situations. 8) Seeking and sharing support. 9) Engagement in our community’s values. 10) Expressing a difference of opinion without directly insulting another user. 11) Please report questionable posts and let the mods deal with it.
.
Helpful Resources
- Are you seeking education, support groups, and more? Take a look at our list of helpful resources.
-
Welcome, mayor!
Welcome to City Hall, here you will find out what’s happening amongst various city builder titles, both new and old. Feel free to discuss with your fellow advisors and mayors, and share your successful and less-than-successful cities alike.
Regional Connections:
- Cities Skylines@lemmy.ml
- Cities Skylines@lemmy.world
- Tycoon
- Workers and Resources
- Dwarf Fortress
- Anno
Rules:
- Memes welcome but keep it within reason.
- Keep this SFW.
- Respect others.
- Be kind always.
Remember, you’re a representative of your city so be on your best behaviour.
-
Lemmy.world Support
Welcome to the official Lemmy.world Support community! Post your issues or questions about Lemmy.world here.
This community is for issues related to the Lemmy World instance only. For Lemmy software requests or bug reports, please go to the Lemmy github page.
This community is subject to the rules defined here for lemmy.world.
To open a support ticket
You can also DM lemmy.world/u/lwreport or email report@lemmy.world (PGP Supported) if you need to reach our directly to the admin team.
Follow us for server news 🐘
Outages 🔥
status.lemmy.world

-
This community is for articles and discussions about the land called Burma or Myanmar.
Myanmar War Map - territories held by different factions fighting for control of Myanmar.
-
DC Cinematic
Enter the dome for news and discussion of DC Films and DC streaming shows, both past and future, animated and live-action alike.
We welcome discussion of DC Elseworlds as well as the DCEU/DCU!
1.) No spoilers in titles and unformatted comments. No spoilers in post titles and spoilers in comments should be formatted correctly.
A spoiler is anything not yet released for home viewing.
A spoiler is not trailers, comics, casting announcements or any other official marketing material.
Comments in [Spoiler] tagged posts do not need to be hidden.
2.) No name calling and general lack of civility. Name calling and general lack of civility will not be tolerated. This is a judgement free zone embracing the subjective nature of film and entertainment. Opinions that do not match your own should be expected.
3.) Don’t be a fanboy or a troll. Definition of a fanboy: A virulent loyalist of a fandom, franchise, or brand. Keep in mind that having a preference, a natural state for fans of any pastime with a form of competition, is not a symptom of fanboyism by itself.
Definition of a troll: A troll makes a habit of deliberately offensive or provocative posting with the aim of upsetting someone or eliciting an angry response from them.
This includes throwaway accounts and usernames composed in bad faith. These may be banned on sight.
4.) Don’t repost. Reposts and articles that do not link back to the original source of news will be removed. Blog posts that discuss and theorize about said news are allowed.
5.) Post on topic. Please only submit posts relating to the DC Extended Universe or other animated/live-action movies based on DC or Vertigo Comics. You can talk about pre-Man of Steel DC movies. This is not a place to discuss animated/live action TV shows not connected to the DCEU/DCU.
6.) Observe proper form with post titles. No spoilers in post titles. Linked articles and videos should be submitted with their original title. When posting other content, the post title should be simple and descriptive. No excessive emoting in post titles, whether in words or emojis. All CAPS titles will be removed. Soapbox post titles (ex. “Wake up, sheeple!” posts) are discouraged. References to voting or karma in a title is grounds for removal. The moderators reserve the right to remove low-quality titles so they can be resubmitted.
7.) Low quality posts will be removed This includes
• Clickbait, fake news, and other sensationalized items.
• Recurring low-effort discussions, such as “Am I the only one who…” posts, redundant worry/concern/hypothetical/soapbox posting
• Posts with titles or bodies that employ hyperbolic/sensational/reactionary language.
• Soapbox posts
• Low-effort memes
• Sourceless “rumors.”
• Thread spam, such as back-to-back posting.
• All final discretion lies with the moderation team.
Based off of: r/DC_Cinematic
-
Infrapolitics is to politics what infrared is to light. Its domain encompasses the acts, gestures, and thoughts that are not quite political enough to be perceived as such.
Learn more here:
-
Skriv et par ord om dig selv og hvad du søger på forummet.
-
A community for discussing science
-
Discussion of all things SEA
- News
- Travel
- Life
en.wikipedia.org/wiki/Southeast_Asia
Rules
- Be nice
- Stay on topic
- Don’t farm rage
- Be respectful of other diets, choices, lifestyles!!!
- No Blanket down voting - If you only come to this community to downvote its the wrong community for you
- No LLM generated posts . Don’t represent machine output as your own, and don’t use machines to burn human response time.
- Brunei
- Cambodia
- Indonesia
- Laos
- Malaysia
- Myanmar
- Philippines
- Singapore
- Thailand
- Timor-Leste
- Vietnam
-
A community for high quality news and discussion around technological advancements and changes
Things that fit:
- New tech releases
- Major tech changes
- Major milestones for tech
- Major tech news such as data breaches, discontinuation
Things that don’t fit
- Minor app updates
- Government legislation
- Company news
- Opinion pieces
-
Cyber Security news and links to cyber security stories that could make you go hmmm. The content is exactly as it is consumed through RSS feeds and wont be edited (except for the occasional encoding errors).
This community is automagically fed by an instance of Dittybopper.
-
Welcome to The Shitpost Office
Shitposts processed from 9 to 5, with occasional overtime on weekends.
Rule 1: Be Civil, Not SinisterTreat others like fellow employees, not enemies in the breakroom.
Rule 2: No Prohibited Postage
- No harassment, dogpiling, or brigading
- No bigotry (transphobia, racism, sexism, etc.)
- Respect people’s time and space. We’re here to laugh, not to loathe
Some packages are simply undeliverable. That means:
- No spam or scams
- No porn or sexually explicit content
- No illegal content
- NSFW content must be properly tagged
If you see anything that violates these rules, please report it so we can return it to sender. Otherwise? Have fun, be silly, and enjoy the chaos. The office runs best when everyone’s laughing… or retching over the stench, at least.
-
Giving you the backstory and appraisals of vintage memes!
Submissions should be vintage memes or commentary about vintage memes. Commenters are advised to appraise the internet value and provenance meme antiquities.
Rules:
- Posts should be old memes or about old memes.
- Don’t be a jerk. Be excellent to each other.
- Keep it safe for work.
- Follow global .world instance rules outlined here
-
This is the Minuteman Missile Computers Users Group. For The Study And Discussion Of Autonetics Designed Computers.
-
RSS Feed of lobste.rs
-
-
A Lemmy community dedicated to Google products and everything Google.
Rules
- Keep it Google.
- Keep it SFW.
-
Europe community on dbzer0. Intended to be a place to discuss European news, politics, or just general topics from a European perspective. Since this is on dbzer0 expect the community to lean more leftist-anarchist but a wide range of views are accepted here (within reason).
Rules:
1. No Bigotry or Hate SpeechAny forms of Homophobia, Transphobia, Queerphobia, Racism, or Ableism will be met with swift and harsh action and will not be tolerated here whatsoever. Bigots will be banned immediately on-sight. This includes apologia of it. Trying to be politely or intellectually bigoted i.e. “Just asking questions” won’t be tolerated.
2. No ZionismAny forms of Zionism or Zionist rhetoric will not be tolerated here, this includes Zionist apologia, accusations of antisemitism towards anti-Zionists, or blatant denial or downplaying of the genocide towards Palestinians. Any attempt to uphold or prop up the IHRA definition of antisemitism, will be treated as Zionism. Anyone engaging in Pro-Zionist sentiment or apologia will be actioned in accordance with its severity. Note: Trying to find loopholes or whataboutery to see what is or isn’t genocide denial or Zionism will be treated as a violation of this rule. Don’t test us.
3. Stay CivilPlease maintain civil discourse in the community. Do not engage in arguments with others, name-calling, or insults. Note that calling out bigotry or Zionism is not considered an insult. In heated arguments users are encouraged to or even required to disengage failure to do so will result in mod action.
4. No MisinformationSpreading of misinformation intentionally in this community is unacceptable and will not be tolerated. Spreading misinformation hurts the credibility of the community and can mislead people sometimes in dangerous ways. Users who intentionally post misinformation as articles, comment answers, or in attempt to win arguments will be actioned swiftly. Note: This includes Russian and Chinese propaganda. Users with a history of such posting will be banned on sight.
5. No AI ContentPlease do not post articles or content primarily created using generative AI. Generative AI content may contain misinformation or be lower quality and thus is discouraged. Posts and comments featuring it will be removed. However this community does not allow or tolerate Anti-AI trolling or hostility and users who engage in such behavior will be actioned for it, additionally Anti-AI trolling violates Rule 3 and often Rule 4 so it is generally unacceptable already.
Note: Rules 1 & 2 may be subject to preemptive mod action due to their severity, and they apply to a user’s entire post history. Not just this community.
-
any and all 1022 related news and content
-
Posts and discussion about comics (and, sometimes, associated media) by the artist centurii-chan.
They have a history of edge-posting - nothing that the current mod considers outright racist, sexist, or otherwise hateful, but problematic enough that you may want to look elsewhere for horny comics.
While you’re here, abide by the following rules or face a ban :
- Don’t be dicks to each other.
- No hate speech, racism, sexism.
- Posts should be related to centuriichan comics.
- Mark NSFW posts as NSFW.
-
The official lemmy community for Voyager, an open source, mobile-first client for lemmy.




Rules
- Be nice.
- lemmy.world instance policy
Sponsor development! 👇


💙
-
A home for the Calisthenics and Bodyweight Fitness!
Whether you’re trying to hit a personal best, get an aesthetic athlete body, starting with strength/body weight training or maybe you’re an expert? Yes!! Ask or post anything related to Calisthenics or Body Weight Training.
🍃🌻 Rule 1: Kindly be empathetic and kind to others. Trolling and spamming will not be tolerated. Making the community a friendly & supportive place is our goal.
All of us are here for a short lifetime. Let’s have a nice time here and avoid negativity. :)
Moderators: @DonaldJMusk ✨
-
Questions, answers, discussions, and literature on the theory and practice of cryptography
Rules (longer version here)
- Stick to cryptography / infosec
- Be a good netizen - be kind, act in good faith, maintain high quality, don’t mislead
- Link directly to original sources
- Don’t use us to cheat on challenges or tests!
- Crypto review requests must show the algorithm
- CTF / challenges and puzzles must use modern crypto
- Avoid making duplicate posts
- All use of AI / LLM and their prompts MUST be disclosed in your submissions and comments
##Related resources;
-
Welcome
This is a safe place to discuss, vent, support, and share information about mental health, illness, and wellness.
Thank you for being here. We appreciate who you are today. Please show respect and empathy when making or replying to posts.
If you need someone to talk to, @therapygary@lemmy.blahaj.zone has kindly given his signal username to talk to: TherapyGary13.12
Rules
The rules for posting and commenting, besides the rules defined here for lemmy.world, are as follows:
- No promoting paid services/products.
- Be kind and civil. No bigotry/prejudice either.
- No victim blaming. Nor giving incredibly simplistic solutions (i.e. You have ADHD? Just focus easier.)
- No encouraging suicide, no matter what. This includes telling someone to commit homicide as “dragging them down with you”.
- Suicide note posts will be removed, and you will be reached out to in private.
- If you would like advice, mention the country you are in. (We will not assume the US as the default.)
If BRIEF mention of these topics is an important part of your post, please flag your post as NSFW and include a (trigger warning: suicide, self-harm, death, etc.)in the title so that other readers who may feel triggered can avoid it. Please also include a trigger warning on all comments mentioning these topics in a post that was not already tagged as such.
Partner Communities
- !ADHD@lemmy.world
- !Autism@lemmy.world
- !Bipolardisorder@lemmy.world
- !Help_Others@lemmy.blahaj.zone
To partner with our community and be included here, you are free to message the current moderators or comment on our pinned post.
-
The community for featuring video media created by Canadian content creators.
This can include youtubers (or youtube adjacent platforms), official documentaries, or even just videos from people vlogging about their experience visiting Canada.
DA RULES
-
Be Respectful: Approach others with kindness and patience. If you have none, offer your silence instead. Discrimination, hate speech, or harassment won’t be tolerated. If you see any, just downvote and report and it will be cleaned up.
-
Stay on Topic: Posts must be relevant to Canadian content creators or Canada in general. A video does not need to be made by a Canadian, so long as it prominently features Canada as a topic in the video.
-
French and English are welcomed: We accept and encourage both official languages. French is super cool. Feel free to post or comment in either language, regardless of the OG post’s language.
-
Content creator promotions: Promotion of the same channel is limited to once a week. The channel must either be Canadian, or the content being shared must feature a Canadian topic prominently in the video. Self-Promos are permitted within this rules as well.
-
Posting Etiquette: The post title MUST include the original video title and the name of the person/entity who published the video. The post must also include a direct link (when possible) of where to watch the video. If you are sharing a channel in general, please include a brief sentence explaining the channel in the title, and elaborate further in the body text. This is very much a show and tell community, don’t just show, tell too!
The No Rules
-
No Memes: No memes, specifically image macro posts. Memes in the comments ARE allowed though.
-
No Political Posts: This community is not the correct place for political discussion. There are better communities on lemmy.ca for that kind of posts that also accept video posts. LGBTQ+ content, in of itself, is not political. For videos that are in a political grey zone, mods reserve the right to use their own discretion.
-
No Pornographic content: No NSFW content. Adult topics are allowed if they are on topic, but adult imagery with the intention of being erotic is not allowed.
-
No Video Game content: Video gaming content is its entirely own pillar of video content creation, that there are other communities more conductive to hosting those posts, such as !canadiangaming@lemmy.ca .
-
No doing stuff that makes me need to make more rules: Moderation reserves the right to take action on anything seen as detrimental to the community. Just because it is not explicitly banned, does not mean it is neccesarily allowed.
Rules are subject to change as the community grows.
-
-
We’re here to help you have a better day! For all wholesome and heartwarming content including memes, news stories, etc.
We chose Reddthat specifically because no downvotes are allowed. Negative comments will be removed.
Please see our twinned community for more wholesome joy…
!dadforaminute@lemmy.world !superbowl@lemmy.world
Rules:
- Be wholesome. Trolling, passive aggressive, nasty comments aren’t allowed.
- No politics. It’s not wholesome.
- Don’t hate on ANY groups. Racist, transphobic, ableist etc comments aren’t allowed.
Positive Communities of Lemmy:
- !goodnewseveryone@piefed.social
- !motivationalmemes@reddthat.com
- !OptimistsUnite@reddthat.com
- !positivity@lemmy.today
-
Memes must be related to phil.
The Memiverse:
!90s_memes@quokk.au
!y2k_memes@quokk.au
!sigh_fi@quokk.au
-
A place to share practical, durable and quality made products that are made to last, with an emphasis on upcycled and sustainable products!
Guidelines:
Things that are well-made and durable (even if they won’t last a lifetime) are A-Okay!
Unlike that other BIFL place, Home-made and DIY items are encouraged here, as long as some form of instruction is included in the body of the post.
Videos links are not allowed as post titles, but you may use them in a text post.
A limited amount of self-promotion is accepted, IF the item you are selling aligns with this criteria:
- The item must be made with sustainable or recycled materials.
- If electronic in some way, the item must be open-source.
- The item must be user-serviceable (if applicable).
- You cannot be a large corporation.
- The post must be clearly marked with a [Self Promotion] tag in your title.
-
Alternative Nation : The Fediverse’s largest alternative and indie music community! All things alternative music, from 80s college rock to today’s indie and all the amazing alternative music in between. Welcome home, music nerds!
Some of y’all may remember MTV’s Alternative Nation or 120 Minutes, awesome programs & incredible ways to discover #music back in the 80s & 90s…
Welcome, to the Fediverse edition!
🎵🎧🎶
Share youtube, songwhip, spotify, bandcamp links, music memes, album art, articles, whatever! But avoid links to directly download music (don’t want to get Lemmy.world in trouble). Songwhip links always appreciated!
See this post on recs on how to post!
The Golden Rule: Music taste is subjective so don’t be a gatekeeping asshole. There’s no “bad music”, only music you like or don’t like.
We Are A Community: So no racism, sexism, homophobia, transphobia, ableism, or spam.
🎵 Let’s get lost in the Fediverse’s record store together! 🎶
Other Lemmy music communities to explore and support:
- !music@lemmy.world
- !90smusic@lemmy.world
- !80smusic@lemmy.world
- !70smusic@lemmy.world
- !60smusic@lemmy.world
- !classicrock@lemmy.world
- !popheads@poptalk.scrubbles.tech
- !HipHopHeads@sopuli.xyz
Where to find ren:
-
Rules
This is an on-topic community. All content must adhere to our CODE OF CONDUCT.
-
For the map enthused!
Rules:
-
post relevant content: interesting, informative, and/or pretty maps
-
be nice
-
-
What’s going on Canada?
Related Communities
🍁 Meta- Main - Lemmy.ca Support - Community Requests
🗺️ Provinces / Territories- Alberta - British Columbia - Manitoba - New Brunswick - Newfoundland and Labrador - Northwest Territories - Nova Scotia - Nunavut - Ontario - Prince Edward Island - Quebec - Saskatchewan - Yukon
🏙️ Cities / Local Communities- Anmore (BC) - Burnaby (BC) - Calgary (AB) - Comox Valley (BC) - Edmonton (AB) - East Gwillimbury (ON) - Greater Sudbury (ON) - Guelph (ON) - Halifax (NS) - Hamilton (ON) - Kingston (ON) - Kootenays (BC) - London (ON) - Mississauga (ON) - Montreal (QC) - Nanaimo (BC) - Niagara Falls (ON) - Niagara-on-the-Lake (ON) - Oceanside (BC) - Ottawa (ON) - Port Alberni (BC) - Regina (SK) - Sarnia (ON) - Saskatoon (SK) - Squamish (BC) - Thunder Bay (ON) - Toronto (ON) - Toronto Cycling - Vancouver (BC) - Vancouver Island (BC) - Victoria (BC) - Waterloo (ON) - Whistler (BC) - Windsor (ON) - Winnipeg (MB) Sorted alphabetically by city name.
🏒 SportsBaseball - Toronto Blue Jays Basketball - Toronto Raptors Curling - Curling Hockey - Main: c/Hockey - list of all Teams - Calgary Flames - Edmonton Oilers - Montréal Canadiens - Ottawa Senators - Toronto Maple Leafs - Vancouver Canucks - Winnipeg Jets Soccer - Main: /c/CanadaSoccer - Toronto FC
💻 Schools / Universities- BC | UBC (U of British Columbia) - BC | SFU (Simon Fraser U) - BC | VIU (Vancouver Island U) - BC | TWU (Trinity Western U) - ON | UofT (U of Toronto) - ON | UWO (U of Western Ontario) - ON | UWaterloo (U of Waterloo) - ON | UofG (U of Guelph) - ON | OTU (Ontario Tech U) - QC | McGill (McGill U) Sorted by province, then by total full-time enrolment.
💵 Finance, Shopping, Sales- Personal Finance Canada - Buy Canadian - BAPCSalesCanada - Canadian Investor - Canadian Skincare - Churning Canada - Quebec Finance - Canada Grown Business
🗣️ Politics- General: - Canada Politics - FairVote Canada - Federal Parties (alphabetical): - Animal Protection Party of Canada - NDP - By Province (alphabetical): - BC Greens
🍁 Social / Culture- 2 North American 4 You (Shitposting & Memes, North America focus) - Ask a Canadian - Bières Québec - Canada Francais - Canadian Gaming - Eh Buddy Hoser (Shitposting & Memes, Canada focus) - EhVideos (Canadian video media) - First Nations - First Nations Languages - Indigenous - Inuit - Logiciels libres au Québec - Maple Music (music)
Rules
- Keep the original title when submitting an article. You can put your own commentary in the body of the post or in the comment section.
Reminder that the rules for lemmy.ca also apply here. See the sidebar on the homepage: lemmy.ca
-
A place to share tips, tools, and experiences from the world of remote work.
-
A handmade home for woodworkers and admirers of woodworkers. Our community icon is submitted by @inquanto@lemmy.world, winner of the Christmas 2025 gift contest with a lovely series of hardwood cutting boards.
-
We keep track of the release of the files, but also to explore what’s already available, and why – with enough exposure – this could bring the man down, and who knows even his regime or the empire.
Want to start digging yourself? Check out our sticky post
Our Rules
(Subject to Change)
- #1 Be kind: keep it civil and amicable. The enemy is not in this community but in Palaces, The White House and penthouses.
- #2 Trigger Warnings: required. Mark posts which may be triggering to read or see for victims of sexual abuse with “[TW]” in front of your post title. If you’re posting an image or video with explicit thumbnail, you will have to set the entire post as NSFW AND include the TW.
- #3 Cite sources: preferably direct link to the article/pdf and or an archive link in case there is a paywalled. In the article find a relevant few paragraphs and quote them in your post.
- #4 Post the Bates numbers: when referencing evidence (even if it is mentioned in an article), please post
- the Bates number of the file you’re referring to (EFTA00000000)
- a link to the original source
- a link to a mirror of the file in case DOJ pulls the file.
- #5 include key paragraphs: when posting articles, include a few key paragraphs of the article (not the entire article)
- #6 avoid links to social media as sources. Links to twitter must use xcancel.com.
Our Justice System
- First offence: warning + 2 day ban
- Second offence: 7 day ban
- Third offence: permanent ban from community
- Creating multiple accounts to interact with this community: permanent ban for all accounts in community + report to your instance admin.
This community is run by volunteers so please don’t test the justice system, as with all justice systems it is critically underfunded.
-
All things pigeon, just no pigeon hate.
Related Communities
!crows@lemmy.ml
!birding@lemmy.world
-
THIS COMM HAS MOVED
!historymemes@piefed.social
-
• Instance rules apply. I forgot to read them, but I’m sure they’re awesome.
• Community is largely random.
• Bullet points are dumb.
-
PoliticoScope — political insights, news, and key global trends. Clear, concise, and unbiased.
-
The future of sustainable transportation is happening today! This is a community for EV owners and enthusiasts. Discuss evolving technology, new entrants, charging infrastructure, government policy, and the ins and outs of EV ownership right here.
Rules
This is an inclusive community. No personal attacks, hate speech, or uncivil behaviour is permitted.
-
Dedicated to the lifter, the runner, the athlete, the dancer, the strong, the fast, the tough, the flexible… the fit.
Rules
Sitewide rules apply. 18+ posts only
Be civil to original posters
Please mark your Original Content with [OC]
Don’t crosspost or repost original content without permission
Self-Promotion is allowed in comments, not in title.
No AI generated images
-
r/startrek: The Next Generation
Star Trek news and discussion. No slash fic…
Maybe a little slash fic.
Rules
1 Be constructiveAll posts/comments must be thoughtful and balanced.
2 Be welcomingIt is important that everyone from newbies to OG Trekkers feel welcome, no matter their gender, sexual orientation, religion or race.
3 Be truthfulAll posts/comments must be factually accurate and verifiable. We are not a place for gossip, rumors, or manipulative or misleading content.
4 Be niceIf a polite way cannot be found to phrase what it is you want to say, don’t say anything at all. Insulting or disparaging remarks about any human being are expressly not allowed.
5 SpoilersUtilize the spoiler system for any and all spoilers relating to the most recently-aired episode. There is no formal spoiler protection for episodes/films after they have been available for approximately one week.
6 Keep on-topicAll submissions must be directly about the Star Trek franchise (the shows, movies, books, etc.). Off-topic discussions are welcome at c/Quarks.
7 MetaQuestions and concerns about moderator actions should be brought forward via DM.
Upcoming Episodes
Date Episode Title 02-19 SFA 1x07 "Ko’Zeine" 02-26 SFA 1x08 "The Life of the Stars" 03-05 SFA 1x09 "300th Night" 03-12 SFA 1x10 "Rubincon" TBA SNW 4x01 TBA
Upcoming Trek
Strange New Worlds (TBA)
Starfleet Academy (TBA)
In Development
Untitled comedy series
Wondering where to stream a series? Check here.
-
COMM MOVED TO !roughromanmemes@piefed.social
-
Pictures, Videos, Articles showing just how boring it is to live in a dystopic society, or with signs of a dystopic society.
Rules (Subject to Change)
–Be a Decent Human Being
–Posting news articles: include the source name and exact title from article in your post title
–If a picture is just a screenshot of an article, link the article
–If a video’s content isn’t clear from title, write a short summary so people know what it’s about.
–Posts must have something to do with the topic
–Zero tolerance for Racism/Sexism/Ableism/etc.
–No NSFW content
–Abide by the rules of lemmy.world
-
-
News and Discussions about Reddit
Welcome to !reddit. This is a community for all news and discussions about Reddit.
The rules for posting and commenting, besides the rules defined here for lemmy.world, are as follows:
Rules
Rule 1- No brigading.**You may not encourage brigading any communities or subreddits in any way. ** YSKs are about self-improvement on how to do things. _____________
:::spoiler Rule 2- No illegal or NSFW or gore content.
**No illegal or NSFW or gore content. **
:::
:::spoiler Rule 3- Do not seek mental, medical and professional help here.
Do not seek mental, medical and professional help here. Breaking this rule will not get you or your post removed, but it will put you at risk, and possibly in danger.
:::
:::spoiler Rule 4- No self promotion or upvote-farming of any kind.
That’s it.
:::
:::spoiler Rule 5- No baiting or sealioning or promoting an agenda.
Posts and comments which, instead of being of an innocuous nature, are specifically intended (based on reports and in the opinion of our crack moderation team) to bait users into ideological wars on charged political topics will be removed and the authors warned - or banned - depending on severity.
:::
:::spoiler Rule 6- Regarding META posts.
Provided it is about the community itself, you may post non-Reddit posts using the [META] tag on your post title.
:::
:::spoiler Rule 7- You can’t harass or disturb other members.
If you vocally harass or discriminate against any individual member, you will be removed.
Likewise, if you are a member, sympathiser or a resemblant of a movement that is known to largely hate, mock, discriminate against, and/or want to take lives of a group of people, and you were provably vocal about your hate, then you will be banned on sight.
:::
:::spoiler Rule 8- All comments should try to stay relevant to their parent content.
:::
:::spoiler Rule 9- Reposts from other platforms are not allowed.
Let everyone have their own content.
:::
:::spoiler Rule 10- Majority of bots aren’t allowed to participate here. This includes using AI responses and summaries.
:::
-
Hi! This is a place for you to share everything positive with kind strangers on the Internet.
Made new friends? Found love? Got a new wonderful job? Bought something cool? Found something amazing on the Internet? Maybe had a wonderful celebration? Maybe something else? Or you’re just in a great, grateful, relaxed mood and want to share some of it with the world?
Share it, and let the fire in your eyes brighten everybody’s day, for joys are best when shared!
Rules:
-
No negativity: This is a safe and positive space. Make sure your posts and comments respect that. If you feel offended by any of the posts - feel free to message admin(s)!
-
No discrimination: Posts and comments should not contain any forms of discrimination and hostilities to any groups of people.
-
No gloating: If you got happier by making someone else feel worse, this is not the place to share it. This is a place to express gratitude, and share moments that will feel warm to everyone.
Rules are work in progress and subject to change. If you want to help moderating the community and keeping it alive, let me (Allero@lemmy.today) know! Everyone is welcome!
-
-
For discussion about electric batteries
-
A community for a webcomic of romance, sarcasm, math, and language.
-
Post a hypothetical scenario.
-
Sometimes we have those little epiphanies in the shower… sometimes they come from other places. This is a home for those epiphanies.
-
A place to share pictures
Rules
1. Images only (obviously).
But meta posts without images are allowed.
2. Pictures only
This community is for pictures. Merriam-Webster defines a picture as “a painting, drawing, or photograph of someone or something.” However, this community will extend this definition. Digital forms such as 3D render are allowed. Abstract art forms that do not represent anything are also allowed.
3. No distracting superimposed text or emoji
Generally, you should be able to appreciate a post without being able to read.
4. No low quality MS paint-esque drawings
5. Remember to follow lemmy.ml sitewide rules
You can find them on the sidebar of the homepage
-
An Irish community in the fediverse.
Check before posting.
If the topic was posted in the last 24 hours, add new articles in the comments of the existing post instead of creating a new one.Link to a genuine source. Screenshots of news articles are only permitted when accompanied by a link. Keep the original headline.
Weather & alerts: www.met.ie
Health Service: www.hse.ie
Central Statistics Office cso.ie
National Broadcasters: www.tg4.ie/en/ • www.rte.ie
Radio Stations: irishradiolive.com
Imeachtaí i nGaillimh feilire.com
Irish Dictionaries: www.focloir.ie/en/ • www.teanglann.ie/en/ • www.potafocal.com/fbg/
Irish language Courses: www.futurelearn.com/courses/irish-language • community-courses.memrise.com/…/english/ • www.duolingo.com/learn
Pollen levels: www.met.ie/forecasts/pollen
-
A place UnSilenced news
Read Full Rules Here!
Rules:
Rules
-
Titles: Video titles must be appropriate and respectful.
-
Misinformation: Do not spread false or misleading information.
-
Civility: Be respectful to other users, even if you disagree with them.
-
Doxxing: Do not post personal information about other users.
-
Threats: Do not make threats of violence or harm against other users.
-
** * Submissions should highlight humanist ideals they also should be about social injustice or subjects that need more exposure. Submissions must not violate the platform’s safety guidelines.
-
Extremism: Do not promote extremist or hateful views.
-
Bad faith: Do not engage in bad faith discussions or arguments.
-
Topic: Stay on topic and avoid derailing discussions.
-
Violence: Do not encourage or promote violence.
-
Dehumanization: Do not justify the dehumanization of any other human being.
-
Medical misinformation: Do not spread false or misleading information about medical topics.
Rule 13: This community is a humanist/leftist community. We promote the advancement of humanity and the betterment of the world. We do not tolerate any form of prejudice or discrimination, and we encourage users to be respectful of each other’s views, even if they disagree
- No complaining about videos not being news videos. Videos are at the discretion of the moderators, and they may remove videos that they deem to be inappropriate or offensive. This includes videos that promote harmful and hateful ideology.
Penalties
Users who violate these rules may be warned, suspended, or banned from the community. The severity of the penalty will depend on the severity of the violation.
-
-
The police problem is that police are policed by the police. Cops are accountable only to other cops, which is no accountability at all.
99.9999% of police brutality, corruption, and misconduct is never investigated, never punished, never makes the news, so it’s not on this page.
When cops are caught breaking the law, they’re investigated by other cops. Details are kept quiet, the officers’ names are withheld from public knowledge, and what info is eventually released is only what police choose to release — often nothing at all.
When police are fired — which is all too rare — they leave with ‘law enforcement experience’ and can easily find work in another police department nearby. It’s called “Wandering Cops.”
When police testify under oath, they lie so frequently that cops themselves have a joking term for it: “testilying.” Yet it’s almost unheard of for police to be punished or prosecuted for perjury.
Cops can and do get away with lawlessness, because cops protect other cops. If they don’t, they aren’t cops for long.
The legal doctrine of “qualified immunity” renders police officers invulnerable to lawsuits for almost anything they do. In practice, getting past ‘qualified immunity’ is so unlikely, it makes headlines when it happens.
All this is a path to a police state.
In a free society, police must always be under serious and skeptical public oversight, with non-cops and non-cronies in charge, issuing genuine punishment when warranted.
Police who break the law must be prosecuted like anyone else, promptly fired if guilty, and barred from ever working in law-enforcement again.
That’s the solution.
♦ ♦ ♦
Our definition of ‘cops’ is broad, and includes prison guards, probation officers, shitty DAs and judges, etc — anyone who has the authority to fuck over people’s lives, with minimal or no oversight.
♦ ♦ ♦
RULES
① Real-life decorum is expected. Please don’t say things only a child or a jackass would say in person.
② If you’re here to support the police, you’re trolling. Please exercise your right to remain silent.
③ Saying
copsANYONE should be killed lowers the IQ in any conversation. They’re about killing people; we’re not.④ Please don’t dox or post calls for harassment, vigilantism, tar & feather attacks, etc.
Please also abide by the instance rules.
It you’ve been banned but don’t know why, check the moderator’s log. If you feel you didn’t deserve it, hey, I’m new at this and maybe you’re right. Send a cordial PM, for a second chance.
♦ ♦ ♦
ALLIES
• r/ACAB
♦ ♦ ♦
INFO
• A demonstrator’s guide to understanding riot munitions
• Cops aren’t supposed to be smart
• Killings by law enforcement in Canada
• Killings by law enforcement in the United Kingdom
• Killings by law enforcement in the United States
• Know your rights: Filming the police
• Three words. 70 cases. The tragic history of ‘I can’t breathe’ (as of 2020)
• Police aren’t primarily about helping you or solving crimes.
• Police lie under oath, a lot
• Police spin: An object lesson in Copspeak
• Police unions and arbitrators keep abusive cops on the street
• Shielded from Justice: Police Brutality and Accountability in the United States
• When the police knock on your door
♦ ♦ ♦
ORGANIZATIONS
• NAACP
• National Police Accountability Project
• Vera: Ending Mass Incarceration
-
A community for news, current events, and overall topics regarding the state of Texas
Other Texas/US Lemmy Communties to follow
Sports
- Houston Astros
- Houston Texans
- Houston Rockets
- Texas Rangers
- Dallas Cowboys
- Dallas Stars
- Austin FC
- San Antonio Spurs
Rules (Subject to Change)
-
Be a Decent Human Being
-
Posting news articles: Please use exact article Titles
-
Posts must have something to do with Texas
-
Zero tolerance for Racism/Sexism/Ableism/etc.
-
No NSFW content
-
Abide by the rules of lemmy.world
-
Sandkasse hvor du kan prøve løs hvordan man bruger forummet. Tråde og posts vil blive fjernet med jævne mellemrum.
-
Share interesting Technology news and links.
Rules:
- No paywalled sites at all.
- News articles has to be recent, not older than 2 weeks (14 days).
- No external video links, only native(.mp4,…etc) links under 5 mins.
- Post only direct links.
To encourage more original sources and keep this space commercial free as much as I could, the following websites are Blacklisted:
- Al Jazeera;
- NBC;
- CNBC;
- Substack;
- Tom’s Hardware;
- ZDNet;
- TechSpot;
- Ars Technica;
- Vox Media outlets(including Axios, due to new changes related to trackers on their website);
- Engadget;
- TechCrunch;
- Gizmodo;
- Futurism;
- PCWorld;
- ComputerWorld;
- Mashable;
- Hackaday;
- WCCFTECH;
- Neowin;
- Jacobin;
- Yahoo;
- Freethink;
- Big Think;
- Newsweek.
More sites will be added to the blacklist as needed.
Encouraged:
- Archive links in the body of the post.
- Linking to the direct source, instead of linking to an article talking about the source.
Misc:
Relevant Lemmy Communities:
-
Games with a space setting, space-focused gameplay or space motifs. Space sims (Elite, Freelancer, X4), space strategy (Stellaris, Star Ruler 2, Moons of Ardan) or even adventure games with a space setting and themes (Citizen Sleeper, Gemini Rue).
Any games about the great beyond.
Some other gaming communities across the Threadiverse:
- Adventure Games - !adventuregames@retrolemmy.com
- Automation Games - !automationgames@lemmy.zip
- Cozy Games - !cozygames@lemmy.world
- City Builders - !citybuilders@sh.itjust.works
- Horror Games (variety) - !horror_games@piefed.world
- Incremental - !incremental_games@incremental.social
- Indie Games (variety) - !bside@fedia.io
- Lifesim Games - !lifesimulation@lemmy.world
- Open Source Games - !foss_gaming@lemmy.world
- PC RPGs (cRPGs) - !crpg@lemmy.world
- Roguelike Games - !roguelikes@lemmy.world
- RTS Games - !rts@reddthat.com
- Strategy Games - !strategy_games@piefed.world
- Turn-based Strategy (4X) - !turnbasedstrategy@piefed.world
- Tycoon / Business Sim Games - !tycoon@lemmy.world
- Video Game Art - !gameart@sopuli.xyz
- Video Game Music - !vgmusic@lemmy.world
- Video Game Questions - !askgaming@piefed.social
Game-specific communities on the Threadiverse:
- Elite - !elitedangerous@lemmy.world
- Kitten Space Agency !kittenspaceagency@sh.itjust.works
- No Man’s Sky - !nomanssky@lemmy.world
- Space Engineers -!spaceengineers@lemmy.zip
Rules (Click to Expand):1) Follow the Piefed.world Rules - https://legal.piefed.world/tos
2) Be kind. No bullying, harassment, racism, sexism etc. against other users.
3) No spam, illegal content, or games with excessive, non-artistic NSFW content (e.g. hentai or porn games).
4) Please stay on topic, focus is on games with a space components and any associated media.
-
A place to share alternatives to popular online services that can be self-hosted without giving up privacy or locking you into a service you don’t control.
Rules:
-
Be civil: we’re here to support and learn from one another. Insults won’t be tolerated. Flame wars are frowned upon.
-
No spam posting.
-
Posts have to be centered around self-hosting. There are other communities for discussing hardware or home computing. If it’s not obvious why your post topic revolves around selfhosting, please include details to make it clear.
-
Don’t duplicate the full text of your blog or github here. Just post the link for folks to click.
-
Submission headline should match the article title (don’t cherry-pick information from the title to fit your agenda).
-
No trolling.
-
No low-effort posts. This is subjective and will largely be determined by the community member reports.
Resources:
- selfh.st Newsletter and index of selfhosted software and apps
- awesome-selfhosted software
- awesome-sysadmin resources
- Self-Hosted Podcast from Jupiter Broadcasting
Any issues on the community? Report it using the report flag.
Questions? DM the mods!
-
-
A community for Sci-Fi themed tabletop RPGs.
Rules
-
No piracy or illegal content. Do not link to, request or encourage piracy or any other illegal content or activities.
-
Stay on-topic. This community is for Sci-Fi tabletop RPGs.
-
Original content. Please only post your own work or make sure you have permission from the original author otherwise.
-
Be civil. Be respectful. Do not incite flamewars, engage in personal attacks, or discriminate in any way.
-
Limit self-promotion. Ask the mods before posting links to your digital products, podcasts, livestreams, or crowdfunding campaigns.
Related communities
Credits
-
-
-
For civil discussion of US politics. Be excellent to each other.
Rule 1-3, 6 & 7 No longer applicable
Rule 4: Keep it civil. It’s OK to say the subject of an article is behaving like a jerk. It’s not acceptable to say another user is a jerk. Cussing is fine.
Rule 5: Be excellent to each other. Posts or comments that are homophobic, transphobic, racist, sexist, ableist, will be removed.
The Epstein Files: Trump, Trafficking, and the Unraveling Cover-Up
Info Video about techniques used in cults (and politics)
Bookmark Vault of Trump’s First Term
-
This is a community for substantive and civil discussion on political topics across the fediverse. If you have a political prompt for discussion, this is your place to ask!
Rules
The rules are simple. Keep it civil, impartial, spam-free, low-effort free and rhetorical-free.
A more detailed, expanded rules based on the princples above is under works. This is a new community and if you are interested in joining our mod team, let us know. (Note, you may only be able to join if you are using mbin, the ability for lemmy users to moderate mbin communities and vice verse is not implemented yet unfortunately)
-
⚓ Dedicated to the discussion of digital piracy, including ethical problems and legal advancements.
Rules • Full Version
1. Posts must be related to the discussion of digital piracy
2. Don’t request invites, trade, sell, or self-promote
3. Don’t request or link to specific pirated titles, including DMs
4. Don’t submit low-quality posts, be entitled, or harass others

Loot, Pillage, & Plunder
We heartily recommend visiting the free port of freemediaheckyeah (aka FMHY) while you sail the high seas, for all the freshest links the ocean has to offer.

📜 c/Piracy Wiki (Community Edition):
Archived🏴☠️ Other communities
FUCK ADOBE!
- !GenP@lemmy.dbzer0.com
Torrenting/P2P:
- !seedboxes@lemmy.dbzer0.com
- !trackers@lemmy.dbzer0.com
- !qbittorrent@lemmy.dbzer0.com
- !libretorrent@lemmy.dbzer0.com
- !soulseek@lemmy.dbzer0.com
Gaming:
- !steamdeckpirates@lemmy.dbzer0.com
- !newyuzupiracy@lemmy.dbzer0.com
- !switchpirates@lemmy.dbzer0.com
- !3dspiracy@lemmy.dbzer0.com
- !retropirates@lemmy.dbzer0.com
💰 Please help cover server costs.


Ko-fi Liberapay
-
A place to talk about parenting.
Be respectful of others’ parenting decisions.
-
There is no such thing as a Stupid Question!
Don’t be embarrassed of your curiosity; everyone has questions that they may feel uncomfortable asking certain people, so this place gives you a nice area not to be judged about asking it. Everyone here is willing to help.
- ex. How do I change oil
- ex. How to tie shoes
- ex. Can you cry underwater?
Reminder that the rules for lemmy.ca still apply!
Thanks for reading all of this, even if you didn’t read all of this, and your eye started somewhere else, have a watermelon slice 🍉.
-
A place for posting anything out of context. Please caption any posts PIC
-
The Discussion on Linux-based Phones.
**Benefits**:- Hardware freedom. - Perfect operating-system competition. - Full utilization of specs. - Phone lifespan raises to 10+ years. - Less e-waste.
**Linux Mobile Distros**:- Ubuntu Touch - Sailfish - FuriOS - Postmarket OS - Mobian - Pure OS - Plasma Mobile - LuneOS - openSUSE Mobile - Nemomobile - Droidian - Mobile NixOS - ExpidusOS - Maemo Leste - Manjaro Arm - Tizen - WebOS
**Linux Mobile Hardware**:- Fairphone 5 - Volla Phone - PinePhone - FLX1 - Librem 5
⚙️Contribute- Ubuntu Touch - Sailfish OS - FuriOS - Postmarket OS - Mobian - Manjaro Arm - Nemo Mobile - Plasma Mobile - LuneOS - Maemo Leste - Librephone
🧼Go Clean From the Duopoly:- !deapple@piefed.social - !deGoogle@lemmy.ca
💻Related Communities:- !linux@programming.dev - !librephone@programming.dev - !alpinelinux@lemmy.ca - !linux4noobs@programming.dev - !linuxvr@lemmy.ca - !privacy@programming.dev
📰News:- Linux Phone Apps - Linux on Mobile
💬Messager:- !matrix@programming.dev - !simplex@programming.dev
⌚️Watch:- !asteroidos@piefed.social - !pinetime@programming.dev
-
This is a place for adult (18+) Lemmy users (lemmings?) to find others with similar interests. Tell us a little about yourself and what kind of lemming(s) you are hoping to find. We also strive to connect people in real life, so if you are seeking a penpal or something similar, this probably is not the place for you.
Formatting your posts helps everybody find what they are looking for quickly, so it will be enforced. <YOUR AGE> [<L4L TAG>] #<LOCATION> - <TITLE>
-
The <L4L TAG> lets lemmings know your gender and that which you are looking for.
- Use either [M]ale or [F]emale based on the anatomy you possess. If you were born with different anatomy than you have currently, add a [T]rans before your current anatomy.
- If you are seeking either [M]ale or [F]emale, use [L]emming.
-
Your <LOCATION> should be a major city/county you are in or near and any state, province, country, or other information that might help other lemmings know where you are geographically. It is best to avoid local abbreviations or slang.
-
Some Examples:
- 20 [M4L] #Chicago - Beantown Bowler Looking to Roll With You
- 35 [TF4M] #Paris - Meet for Crepes at the Eiffel Tower and Walk Along the Seine
- 78 [M4F] #Paradise Falls - Roommate Wanted. Must Love Balloons, Dogs, and Adventure.
NSFW or commercial material of any kind is NOT allowed here.
-
-
- Please include the health status (alive, not alive) in the title of your post.
- Behave.
-
A community to discuss space & astronomy through a STEM lens
Rules
- Be respectful and inclusive. This means no harassment, hate speech, or trolling.
- Engage in constructive discussions by discussing in good faith.
- Foster a continuous learning environment.
> Please keep politics to a minimum. When science is the focus, intersection with politics may be tolerated as long as the discussion is constructive and science remains the focus. As a general rule, political content posted directly to the instance’s local communities is discouraged and may be removed. You can of course engage in political discussions in non-local communities.
Related Communities
🔭 Science- !curiosityrover@lemmy.world - !earthscience@mander.xyz - !esa@feddit.nl - !nasa@lemmy.world - !perseverancerover@lemmy.world - !physics@mander.xyz - !space@beehaw.org
🚀 Engineering- !rocketlab@lemmy.nz - !spaceflight@sh.itjust.works - !spacex@sh.itjust.works
🌌 Art and Photography- !astrophotography@lemmy.world - !thenightfeeling@lemmy.world
Other Cool Links
-
From video gaming to card games and stuff in between, if it’s gaming you can probably discuss it here!
Please Note: Gaming memes are permitted to be posted on Meme Mondays, but will otherwise be removed in an effort to allow other discussions to take place.
See also Gaming’s sister community Tabletop Gaming.
This community’s icon was made by Aaron Schneider, under the CC-BY-NC-SA 4.0 license.
-
Post links to futurology content on Youtube you would like to share.
-
-
A community to discuss fruit trees, fruit forestry, fruitarianism, and all things fruit-related.
Post photos of your fruit trees or harvests, share growing information or interesting articles, ask questions, or just express your appreciation for fruit in general!
No anti-fruit posts/comments. Let’s keep this a positive space!
Banner photo of Pereskia aculeata by Lumicon (CC BY-SA 4.0)
-
Welcome to Formula1 @ lemmy.world Lemmy’s largest community for Formula 1 and related racing series
📆 F1 Calendar
🏁 FIA Documents
📊 F1 Pace
2026 Calendar
Location Date 🇲🇨 Monaco 05-07 Jun 🇪🇸 Spain 12-14 Jun 🇦🇹 Austria 26-28 Jun 🇬🇧 Great Britain 03-05 Jul 🇧🇪 Belgium 17-19 Jul 🇭🇺 Hungary 24-26 Jul 🇳🇱 Netherlands 21-23 Aug 🇮🇹 Italy (Monza) 04-06 Sep 🇪🇸 Barcelona-Catalunya 11-13 Sep 🇦🇿 Azerbaijan 24-26 Sep 🇸🇬 Singapore 09-11 Oct 🇺🇸 USA (Austin) 23-25 Oct 🇲🇽 Mexico 30 Oct-01 Nov 🇧🇷 Brazil 06-08 Nov 🇺🇸 USA (Las Vegas) 19-21 Nov 🇶🇦 Qatar 27-29 Nov 🇦🇪 Abu Dhabi 04-06 Dec Rules
1. Be respectful.
Treat drivers, teams, and fellow Lemmings with respect. Healthy debate is encouraged, but keep it civil and constructive.2. No duplicate news.
Please check the feed before posting. Multiple posts from different news companies reporting the exact same thing will be removed to keep the feed clean.3. Spoilers.
This is a live sports community. We discuss sessions in real-time, so browse at your own risk during race weekends!4. Make content accessible.
• Non-English articles: Include a translated summary (e.g., DeepL).
• Paywalled articles: Provide a brief summary in the comments.5. Social media.
Post social media updates as screenshots so everyone can view them without needing an account. Always include the original source link.6. Zero tolerance for spam. Strictly no gambling, crypto, or NFT-related content.
-
A place to discuss the TV show Farscape
-
Simplifying Complexity, One Answer at a Time!
Rules
- Be respectful and inclusive.
- No harassment, hate speech, or trolling.
- Engage in constructive discussions.
- Share relevant content.
- Follow guidelines and moderators’ instructions.
- Use appropriate language and tone.
- Report violations.
- Foster a continuous learning environment.
-
A UK-centric Electric Vehicles community, where discussion/news of the wider European continent is welcome.
All discussion of EVs (and hybrids for the moment), charging networks, etc, welcome!
No USA/Americas news unless it is relevant to the UK/Europe - most of the existing EV communities on Lemmy are awash with US discussion, please use one of those. US news and discussion will be removed.
The main “global” EV community is !electricvehicles@slrpnk.net
-
Inspired by the Dull Men’s Club.
1. Relevant commentary on your own dull life. Posts should be about your own dull, lived experience. This is our most important rule. Direct questions, random thoughts, comment baiting, advice seeking, many uses of “discuss” rarely comply with this rule.
2. Original, Fresh, Meaningful Content.
3. Avoid repetitive topics.
4. This isn’t an advice forum
Use a search engine, a tradesperson, Reddit, friends, a specialist Facebook group, apps, Wikipedia, an AI chat, a reverse image search etc. to answer simple questions or identify objects. Also see rule 1, “comment baiting”.
There are a number of content specific communities with subject matter experts who can help you.
Some other communities to consider before posting:
5. Keep it dull. If it puts us to sleep, it’s on the right track. Examples of likely not dull: jokes, gross stuff (including toes), politics, religion, royalty, illness or injury, killing things for fun, or promotional content. Feel free to post these elsewhere.
6. No hate speech, sexism, or bullying No sexism, hate speech, degrading or excessively foul language, or other harmful language. No othering or dehumanizing of anyone or negativity towards any gender identity.
7. Proofread before posting. Use good grammar and punctuation. Avoid useless phrases. Some examples: - starting a post with “So” - starting a post with pointless phrases, like “I hope this is allowed” or “this is my first post” Only share good quality, cropped images. Do not share screenshots of images; share the original image.
-
Drugs discussion community.
-
A place for those looking to get away from the traditional cable tv model, and move toward cheaper and legal options like over the air antenna, library collections, and streaming services.
-
Typical internet cats. Videos, pics, memes, and discussion welcome!
Rule 1) Be kind
Rule 2) Follow the lemmy.world rules
other cat communities
birds, some cats
-
Welcome! 🤖
Our community focuses on programming-oriented, hype-free discussion of Artificial Intelligence (AI) topics. We aim to curate content that truly contributes to the understanding and practical application of AI, making it, as the name suggests, “actually useful” for developers and enthusiasts alike.
Be an active member! 🔔
We highly value participation in our community. Whether it’s asking questions, sharing insights, or sparking new discussions, your engagement helps us all grow.
What can I post? 📝
In general, anything related to AI is acceptable. However, we encourage you to strive for high-quality content.
What is not allowed? 🚫
- 🔊 Sensationalism: "How I made $1000 in 30 minutes using ChatGPT - the answer will surprise you!"
- ♻️ Recycled Content: “Ultimate ChatGPT Prompting Guide” that is the 10,000th variation on "As a (role), explain (thing) in (style)"
- 🚮 Blogspam: Anything the mods consider crypto/AI bro success porn sigma grindset blogspam
General Rules 📜
Members are expected to engage in on-topic discussions, and exhibit mature, respectful behavior. Those who fail to uphold these standards may find their posts or comments removed, with repeat offenders potentially facing a permanent ban.
While we appreciate focus, a little humor and off-topic banter, when tasteful and relevant, can also add flavor to our discussions.
Related Communities 🌐
General
- !Artificial@kbin.social
- !artificial_intel@lemmy.ml
- !singularity@lemmy.fmhy.ml
- !ai@kbin.social
- !ArtificialIntelligence@kbin.social
- !aihorde@lemmy.dbzer0.com
Chat
Image
Open Source
Please message @sisyphean@programming.dev if you would like us to add a community to this list.
Icon base by Lord Berandas under CC BY 3.0 with modifications to add a gradient
-
About
A community for the most based memes from atheists, agnostics, antitheists, and skeptics.
Rules
-
No Pro-Religious or Anti-Atheist Content.
-
No Unrelated Content. All posts must be memes related to the topic of atheism and/or religion.
-
No bigotry.
-
Attack ideas not people.
-
Spammers and trolls will be instantly banned no exceptions.
-
No False Reporting
-
NSFW posts must be marked as such.
Resources
International Suicide Hotlines
Non Religious Organizations
Freedom From Religion Foundation
Ex-theist Communities
!exchristian@lemmy.one
!exmormon@lemmy.world
!exmuslim@lemmy.world
Other Similar Communities
!religiouscringe@midwest.social
!priest_arrested@lemmy.world
!atheism@lemmy.world
!atheism@lemmy.ml
-
-
A community to satirize conservtive and right-wing “ideals”.
This community (now) exists as a pressure valve, a place to process through humor the often frustrating world of conservative politics. Above all, this is NOT the place for serious conservative support/viewpoints/arguments. There are other places on Lemmy for that if you desire it.
Rules:
-
Always follow .world instance rules
-
Parody With Purpose: This is a space for humorous takes on conservative politics. We welcome satire, but draw the line at content that promotes racism, sexism, homophobia, or other forms of bigotry.
-
Memes Over Manifestos: This community focuses on humor and parody, not serious political debate. There are plenty of spaces for earnest conservative discussion, this isn’t one of them.
-
Highlight Contradictions: Sometimes the best content points out inconsistencies and hypocrisies in conservative talking points. Creative commentary is encouraged.
-
Public Figures Fair Game: Politicians and pundits can be satirized, but no targeting of private individuals, doxxing, or harassment.
Children of public figures under the age of 14 are also off-limits, a 16 year old has enough free agency to break with or adopt their parents views. An 8 year old kid doesn’t.
-
No News Zone: Memes only, news or other serious content should be sent to the nearest relevant comm. Meme’s of current events, however, are encouraged.
-
Clear Satire: Make your satirical intent reasonably clear. We’re here to mock bad ideas, not accidentally spread them. If you’re unsure how it will be taken, feel free to DM the mod team ahead of time or explicitly tag it as satire in the body.
A note on ChadMcTruth: Chad’s content is 100% satire, but his work can sometimes be hard to tell, but if he posted it be assured, its satire.
- Relevant Content: All posts should relate to conservative politics or ideologies in some way somewhere in your post. Either in the title or the meme itself.
For more general political memes please see !politicalmemes@lemmy.world
-
Community Respect: Disagree with fellow members all you want, but personal attacks aren’t welcome. Save the criticism for the ideas, not each other.
-
Moderation Discretion: Mods will use reasonable judgment in applying these rules. We’ll be fair, but firm. These kinds of comms have a tendency to get off the rails, so we might seem overzealous in moderation sometimes.
-
For the moment, i’m allowing properly tagged NSFW content as long as its funny and relevant. Don’t make me regret it.
And above all, HAVE FUN!
-
-
Storage place for my improvisations
-
Discussion of EVs and the technology around them
-
Hello there. Somehow, Star Wars memes have returned. It’s not a trap, this is where the fun begins.
==========
Other universes to visit:
!lotrmemes@midwest.social
!tenforward@lemmy.world
Separatist systems:
!prequelmemes@lemmy.world
Oh hey some real SW content for a change (perhaps):
!star_wars@lemmy.world
!starwars@lemmy.ml
!starwarstelevision@lemmy.world
==========
IMPORTANT
Please do not post the “good friend” or similar copypasta
==========
Our galactic citizens have requested more specific rules, so here are a few.
The general idea is, if you’re looking here for rules, you’re probably someone who doesn’t need to have them spelled out. You’re fine. But anyway:
-
This is a community for Star Wars memes. This means typically screenshots of Star Wars media with some text or context that’s meant to be funny and/or thoughtful. All SW media is welcome: movies, games, comic books, fanart… Other kinds of content, like video links or meta memes (about this community, or Lemmy), are fine as well, just keep it on topic.
-
We are all friends here, and love (sometimes love to hate) Star Wars. Be nice to each other.
-
As fans of fictional media, we can be passionate. If you very strongly disagree with something or someone, take a deep breath before reacting. Anger leads to the dark side!
-
Everything in Star Wars has happened a long time ago, in a galaxy far away, and it’s a rich universe of millions of words and millions of years of history. So current Earthly matters really shouldn’t concern us here. In other words, leave politics, philosophies and convictions behind the door. This applies even if it’s about something related to Star Wars.
-
Original content is preferred. Reposts are fine, just please limit to a maximum of 3 per day, per citizen. It is recommended, but not required, to mark original memes as (OC) and reposts as (repost).
-
Local mods are the Jedi council. They may take actions that are necessary to maintain peace and stability of the Republic, even beyond the rules outlined here. Follow their guidance.
-
Regular rules of the Lemmy.world instance apply.
-
-
Responses that completely destroy the original argument in a way that leaves little to no room for reply - a targeted, well-placed response to another person, organization, or group of people.
The following things are not grounds for murder:
- Personal appearance (“You’re fat”, “You’re ugly”)
- Posts with little-to-no context
- Posts based on a grammar/spelling error
- Dick jokes, “Yo mama”, “No, you” type responses and other low effort insults
- "Your values are bad" without any logcal or factual ways of showing that they are wrong (“I believe in capitalism” - “Well, then you must be evil” or “Fuck you you ignorant asshole”)
Rules:
- Be civil and remember the human. No name calling or insults. Swearing in general is fine, but not to insult someone else.
- Discussion is encouraged but arguments are not. Don’t be aggressive and don’t argue for arguments sake.
- No bigotry of any kind.
- Censor the person info of anyone not in the public eye.
- If you break the rules you’ll get one warning before you’re banned.
- Enjoy the community in the light hearted way it’s intended.
-
This is a community for posting and sharing trailers and teasers for upcoming film, television and video game premieres. The goal is to provide subscribers a curated feed of trailers for UPCOMING media. General-purpose posts about movies, television and games are better suited for other communities around the Lemmyverse. This place is just for trailers.
Rules
- All posts must be trailers or teasers; not full movies, not trailers for trailers, and not clips of popular scenes. Meta posts from mod staff are OK, but should be kept to a minimum.
- No fan-made trailers or remixes.
- Trailers for upcoming content only and not reposts. Do not spam the community with trailers for media that has already been released or by reposting the same media multiple times.
- Link to official channels for trailers whenever possible (ie: the YouTube accounts of each film’s studio or distribution company); avoid linking to videos from media outlets that function as aggregators / re-posters if you can.
- Post titles should follow formatting guidelines: “Media Name (release year, relevant creator credit)”. Creator credits should be directors for films and games, showrunners for television series. Other details such as starring actors, writers, production studios, etc can be added to the post description.
- Don’t be a jerk.
-
Reviews of all passively consumable media (books, movies, shows, youtube, etc).
Only reviews! No trailers, teasers, gossip, speculation, behind the camera drama, anything meta.
Rules
0 - Reviews only!
- Be nice
- Stay on topic
- Don’t farm rage
- No Blanket down voting
-
Welcome to New Brunswick’s home on Lemmy!
-
No bigotry - including racism, sexism, ableism, homophobia, transphobia, or xenophobia.
-
Be respectful. Everyone should feel welcome here.
-
No porn.
-
No ads / spamming.
Bienvenue à la communauté néo-brunswickoise de Lemmy!
-
Pas d’intolérance - y comprit le racisme, le sexisme, le capacitisme, l’homophobie, la transphobie, ou la xénophobie.
-
Soyez respectueux•ses. Tous•tes devrait se sentir bienvenue ici.
-
Aucune pornographie.
-
Pas de promotion / spam.
Related communities / Communautés similaires
This is a bilingual community, feel free to participate in either French or English (or even in chiac!)
//
On est une communauté bilingue, soyez à l’aise de participer en anglais ou en français (ou même en chiac!)
-
-
A place for questions.
-
Memes about the Fediverse.
Rules
General
- Be respectful
- Post on topic
- No bigotry or hate speech
- Memes should not be personal attacks towards other users
- We are not YPTB. If you have a problem with the way an instance or community is run, then take it up over at !yepowertrippinbastards@lemmy.dbzer0.com.
- Addendum: Yes we know that you think ml/hexbear/grad are tankies and or .world are a bunch of liberals but it gets old quickly. Try and come up with new material.
- This is not the place to start flamewars between Lemmy, Mbin and Piefed.
Elsewhere in the Fediverse
Other relevant communities:
- !fediverse@lemmy.world
- !yepowertrippinbastards@lemmy.dbzer0.com
- !lemmydrama@lemmy.world
- !fediverselore@lemmy.ca
- !bestofthefediverse@lemmy.ca
- !fedigrow@lemmy.zip
-
A community dedicated to the weirdest people involved in politics.
- Focus on weird behaviors and beliefs
- Follow Iemmy.world TOS
- Don’t be a jerk
-
-
General OpenBSD community!
-
This community is for support requests specific to lemmy.ca.
If you need to contact an admin privately, please message @admin@lemmy.ca.
If you are a technical user and you have questions or need support with the Lemmy software itself, please visit !lemmy_support@lemmy.ml.
-
한국에 관심 있는 모두를 위한 공간 / Space for everyone interested in everything Korean
-
-
Discuss how to save money.
-
A Lemmy community for the game Factorio made by Wube Software.
Rules
- Be a good person
- Content must relate to Factorio
- Adhere to Lemmy’s Code of Conduct
-
-
For sharing interesting videos from around the Web!
Rules
- Videos only (aside from meta posts flagged with [META])
- Follow the global Mastodon.World rules and the Lemmy.World TOS while posting and commenting.
- Don’t be a jerk
- No advertising
- No political videos, post those to !politicalvideos@lemmy.world instead.
- Avoid clickbait titles. (Tip: Use dearrow)
- Link directly to the video source and not for example an embedded video in an article or tracked sharing link.
- Duplicate posts may be removed
- AI generated content must be tagged with “[AI] …” ^Discussion^
Note: bans may apply to both !videos@lemmy.world and !politicalvideos@lemmy.world
-
A place for all kinds of scent heads. Post just about anything related to perfumes (eg. ask for recommendations, help finding a fragrance or simply share what you’re currently wearing)
📍Rules:
- Be nice
- No scams, no spam
- Follow instance rules
-
Moving the lemm.ee State Level Doge community here and giving it a broader name.
The lemm.ee community was originally created to track the “DOGE task forces” which popped up across multiple states in the U.S. once Trump took office in 2025, but is meant to be a place for anyone, anywhere to share and discuss any corruption they notice happening at a local/community level.
Rules:
Be respectful
No abusive language
No bigotry
No ads
No porn
-
Community dedicated to memes that often hit a little too close to home. Respect the instance rules and remember that sharing these memes with your SO might 50/50 put you in the doghouse.
-
This is a community to discuss the housing crisis in Canada.
All so Canadians can find a decent home to live in.
Racism is still absolutely prohibited, but you are welcome to debate population growth, immigration rate, foreign home buyers, and the merits of single family homes or the green zone.
A merge of r/canadahousing and r/canadahousing2 for those coming from Reddit.
Bits of the sidebar and logo taken from those subs and will be going through a slight revision as things get settled.
-
Overview:
The Lemmy place to discuss the news and experiences of transgender people.
**Rules:**1. Keep discussions civil. 2. Arguments against transgender rights will be removed. 3. No bigotry is allowed - including transphobia, homophobia, speciesism, racism, sexism, classism, ableism, castism, or xenophobia.
**Related:**!lgbtq_plus@lemmy.blahaj.zone !intersex@lemmy.blahaj.zone
-
The new home of /r/Android on Lemmy and the Fediverse!
Android news, reviews, tips, and discussions about rooting, tutorials, and apps.
🔗Universal Link: !android@lemdro.id
💡Content Philosophy:
Content which benefits the community (news, rumours, and discussions) is generally allowed and is valued over content which benefits only the individual (technical questions, help buying/selling, rants, self-promotion, etc.) which will be removed if it’s in violation of the rules.
Support, technical, or app related questions belong in: !askandroid@lemdro.id
For fresh communities, lemmy apps, and instance updates: !lemdroid@lemdro.id
📰Our communities below
Rules
-
Stay on topic: All posts should be related to the Android OS or ecosystem.
-
No support questions, recommendation requests, rants, or bug reports: Posts must benefit the community rather than the individual. Please post to !askandroid@lemdro.id.
-
Describe images/videos, no memes: Please include a text description when sharing images or videos. Post memes to !androidmemes@lemdro.id.
-
No self-promotion spam: Active community members can post their apps if they answer any questions in the comments. Please do not post links to your own website, YouTube, blog content, or communities.
-
No reposts or rehosted content: Share only the original source of an article, unless it’s not available in English or requires logging in (like Twitter). Avoid reposting the same topic from other sources.
-
No editorializing titles: You can add the author or website’s name if helpful, but keep article titles unchanged.
-
No piracy or unverified APKs: Do not share links or direct people to pirated content or unverified APKs, which may contain malicious code.
-
No unauthorized polls, bots, or giveaways: Do not create polls, use bots, or organize giveaways without first contacting mods for approval.
-
No offensive or low-effort content: Don’t post offensive or unhelpful content. Keep it civil and friendly!
-
No affiliate links: Posting affiliate links is not allowed.
Quick Links
Our Communities+ !askandroid@lemdro.id + !androidmemes@lemdro.id + !techkit@lemdro.id + !google@lemdro.id + !nothing@lemdro.id + !googlepixel@lemdro.id + !xiaomi@lemdro.id + !sony@lemdro.id + !samsung@lemdro.id + !galaxywatch@lemdro.id + !oneplus@lemdro.id + !motorola@lemdro.id + !meta@lemdro.id + !apple@lemdro.id + !microsoft@lemdro.id + !chatgpt@lemdro.id + !bing@lemdro.id + !reddit@lemdro.id
Lemmy App List Chat and More+ Android Chat + Lemdro.id Chat + Mods Chat + Lemdro.id Admin Chat + Reddit
-
-
This is a community for news, discussion and media regarding the international mutual aid network of collectives called food not bombs. Share images, recipes, and advice. Find resources, local branches, or learn how to start your own group. Food is a human right.
-
Welcome to /c/Tumblr
All the chaos of Tumblr, without actually going to Tumblr.
Rule 1: Be Civil, Not CursedThis isn’t your personal call-out post.
Rule 2: No Forbidden Posts
- No harassment, dogpiling, or brigading
- No bigotry (transphobia, racism, sexism, etc.)
- Keep it fun and weird, not mean-spirited
Some things belong in the drafts forever. That means:
- No spam or scams
- No porn or sexually explicit content
- No illegal content (don’t make this a federal case)
- NSFW screenshots must be properly tagged
If you see a post that breaks the rules, report it so the mods can handle it. Otherwise just reblog and relax.
-
Anything and everything goes: Memes, Jokes, Vents, and Banter. The limitations on content here are pretty lax, and we primarily rely on voting to determine what people want to see, but if there is an obvious problem (rules below), mods will intervene.
Rules:
1. No harrassment or hateful language
Don't use hateful language directed toward a group of people. Don't harrass other users.
...
2. No Illegal Content
Content that violates the law. Any post/comment found to be in breach of common law will be removed and given to the authorities if required.
That means:
-No promoting violence/threats against any individuals
-No CSA content or Revenge Porn
-No sharing private/personal information (Doxxing)
...
3. No Spam
-If you have posted content, please refrain from re-posting said content within this community.
-Do not spam posts with intent to harass, annoy, bully, advertise, scam or harm this community.
-No posting Scams/Advertisements/Phishing Links/IP Grabbers
-No Bots, Bots will be banned from the community.
...
4. No Porn/ExplicitContent
-Do not post explicit content.
-Do not post Gore or Shock Content.
...
5. No Enciting Harassment, Brigading, Doxxing or Witch Hunts
-Do not Brigade other Communities
-No calls to action against other communities/users.
-No Witch Hunts against users/communities.
-No content that harasses members within or outside of the community.
...
-
For [Blue|Purple] Teams in Cyber Defence - covering discovery, detection, response, threat intelligence, malware, offensive tradecraft and tooling, deception, reverse engineering etc.
-
Welcome to Weightroom
Weightroom is a community for barbell and dumbbell strength and hypertrophy training, including powerlifting, beginner routines, conditioning and serious gym progress.
Start Here: TheFitness.Wiki
The best beginner-friendly resource, curated from /r/Fitness and /r/Weightroom.
Recommended reading:
Muscle building 101
Weight loss 101
RoutinesRecommended apps:
Weekly Threads:
Weekly training logs - Monday
Weekend questions - FridayRules:
Be respectful. Everyone starts somewhere
For general fitness check out !fitness@lemmy.world
-
Have a question about a fictional universe? Ask it here!
Rules
1-Please tag your post with the fictional universe you are asking about. e.g. [Star Wars] or [Marvel Cinematic Universe].
2-Only questions about fiction are allowed. Real-world questions are better suited for a question and answer community
3-Any fiction is allowed, not just science fiction. General questions not related to one specific universe are allowed.
4-Roleplaying is not mandatory, but all answers should ideally be framed from the perspective of the fictional universe being asked about.
5-Above all else, be kind and considerate to others. Remember, if you are not building this community up, you are tearing it down.
-
-
A community for weight-loss, primarily by means of inducing a caloric deficit.
-
Das Sammelbecken auf feddit.org für alle Deutschsprechenden aus Deutschland, Österreich, Schweiz, Liechtenstein, Luxemburg und die zwei Belgier. Außerdem natürlich alle anderen deutschprechenden Länderteile der Welt.
Für länderspezifische Themen könnt ihr euch in folgenden Communities austauschen:
___
Zusätzliche Regeln aus „Lessons learned":
- Postet hier zu allen Themen, die euch interessieren (soweit sie den anderen Regeln genügen)
- Posts oder Antworten, die einen Archive[.]today (oder eines der Derivate) beinhaltet, werden kommentarlos gelöscht
- Es werden Posts zum Thema Nahost / Palästina/Israel hier auf Dach gelöscht.
- Dasselbe gilt für Wahlumfragen à la Sonntagsumfrage.
- Bitte Titel von Posts nur sinnerweiternd und nicht sinnentstellend verändern. Eigene Meinungen gehören in den Superkommentar oder noch besser in einen eigenen Kommentar darunter.
- Youtube Videos bitte nicht ohne eine zusätzliche Zusammenfassung posten
___
Einsteigertipps für Neue gibt es hier.
___Eine ausführliche Sidebar mit den Serverregeln usw. findet ihr auf der Startseite von feddit.org
___
-
For all things ereader

















A world of content at your fingertips…
Think of this as your global discovery feed. It brings together interesting discussions from across the web and other communities, all in one place.
While you can browse what's trending now, the best way to use this feed is to make it your own. By creating an account, you can follow specific creators and topics to filter out the noise and see only what matters to you.
Ready to dive in? Create an account to start following others, get notified when people reply to you, and save your favorite finds.
Register Login-
ANXIOUS MOTHER (PERFORATED APPENDIX)
STEM - You are a surgical SHO on call for emergency general surgical admissions. A 10-year-old girl Sarah was brought by her neighbour as an emergency with peritonitis, Her mother was at work when she was told that her daughter is in hospital.
The child Sarah, is febrile and extremely ill, A perforated appendix is suspected and she is being resuscitated by your registrar before being taken to the operating theatre. You've just arrived in the hospital for your shift and haven't seen the patient. Your consultant, Mr, Mann is on his way from home, and will perform the operation, She became anxious when she realize that Mr. Mann is the same surgeon who operated upon her husband and couldn't save his life.
Considering this communication skills station, you are asked to talk to this anxious mother and answer her queries.
Doctor: Hello, good evening, I'm Dr. Z, one of the surgical doctors. Am I talking to Sarah's mother? *Patient: It's not a good evening for me, doctor, at all. What's going on here? All of you have taken my child for an operation even without letting me know. How is this even possible?* Doctor: I was told to speak with you about your child condition. Can we please have a seat so that we can discuss about everything a bit more detailed? Could you first tell me what do you know so far? *Patient: My child had fever from yesterday; but still I went to my work. I have no clue, doctor. It's all happened because of not being in home.* Doctor: First, you don't have to feel guilty because this could happen anyway. Your daughter was brought by your neighbour complaining of tummy pain. Our initial investigation revealed the suspicion of acute appendicitis. She was managed by our registrar and received some TV fluids and antibiotics. We are now waiting for theconsultant who will operate upon her. *Patient Are you sure that my daughter has acute appendicitis?* Doctor: We are suspecting acute appendicitis as this is common condition and also her signs and symptoms denotes this. But we cannot be certain 100% until we open and see. Usually we do a keyhole first, then look for it. Then after observation we complete the procedure. if it ruptures and case general infection of your tummy, or if this failed, we need to convert it to open appendectomy by giving a small incision over right lower tummy. *Patient: Is it dangerous, doctor?* Doctor: In children specifically, there is less fat inside the abdomen, so perforation can be particularly dangerous. In such case your child may go to a higher care area called HDU. But Mr. Mann is a very good surgeon, I can assure you that your childis in very good hands. We will be looking after her but there are still some concerns. *Patient: Will the wound be disfiguring?* Doctor: A small horizontal wound will leave a little scar, but we may need to expand the wound and this may leave a bigger scar. We will try to make as little scar as possible. / As she is a girl, it's conecrning, but still we will try to make it as short as possible. *Patient: Is there any other problem that could occur?* Doctor: Yes, probably severe infection can block the reproductive tubes in young girls, so future sub fertility may happen. *Patient: Do you mean that she can’t get pregnant in the future?* Doctor: I understand your apprehension, no need to worry because she has another fine working tube on the other side. *Patient But Mr, Mann did operation for my husband, and he died,* Doctor: I am so sorry to hear that. Please accept my sincere condolences. May I ask when and how he died? *Patient: Mr. Mann did operation for him because he had colon cancer and he died few weeks after the operation at home.* Doctor I am so sorry to hear that again. I think those are two different situations. I think your husband died from the cancer not the surgery and Mr. Mann one of best surgeon we have in the hospital who has a vast experience on this, we will take good care of your daughter. *Patient: Can I change the consultant?* Doctor: Of course, you can because it's within your rights. But it’s time consuming as the new consultant will study the case from the beginning. As i's a suirgical emergency it will have a deleterious impact on your child health. So, I will not recommend you do that. *Patient: Can I see her?* Doctor: Obviously, you can see her. But she will be kept in observational room just after the operation. Once she regains her consciousness, you can definitely see her. Do you have any other concerns? *Patient: I just need to be everything ok for my child.* Doctor: Of course, my team is trying our best. Lets summarize what we have been through here. Your child has been brought here by your neighbour complaining of tummy pain. Our initial investigation revealed acute appendicitis and we are now waiting for the consultant to operate upon her, and I’ve explained the risks and benefits of this operation. We all are here to help and support you and to dive you a hand at any time. Should there be any concerns, please don’t hesitate to contact me at any moment. I will leave my bleep number at the nurse station. Thank you so much for your co-operation.
-
STEM 1 - You are asked to take the history John, a middle-aged male on the 5th post-op day who has presented with low mood for 6 hours and loss of appetite. He is not willing to talk to anyone and seems to be lost, The nursing staff informs you that he has been sleeping poorly post-operatively.
PRESENTATION John, a 56-year-old occupation, previously fit/smoker/social drinker who is on his 5th POD following ... [e.g. right hemicolectomy], has showed signs of anhedonia, depression and fatigue. He has also showed some signs of positive core biological symptoms. Considering all of this, my provisional diagnosis is reactive (postoperative depression), I will also consider major depressive disorder, bipolar disorder. What will be your management? For mild condition Regular exercise Advice on sleep hygiene (regular sleep times, appropriate environment) = Psychosocial therapy -CBT Moderate to severe Regular exercise, advice on sleep hygiene CBT Medication -SSRIs High-intensity psychosocial intervention (CBT or interpersonal therapy) Immediate and considerable high risk to themselves or others: Admit to psychiatric ward (use Mental Health Act if necessary) -
Stem:
You are the surgical SHO working in the general surgery department 4G ward at St Bartholomew’s hospital, London. Mrs. Eleanor Thompson, DOB: 15/06/1942 has been admitted for right-sided simple mastectomy and axillary lymph node clearance, the operation is uneventful, and a drain is inserted, postoperatively she has developed axillary swelling, discomfort and is short of breath, please update the consultant Mr. Mann about her current condition and ask for advice.
S — Situation “Hello, it’s David, the SHO on Ward 4G. I’m calling about Mrs Eleanor Thompson, DOB 15/06/1942, who is post-operative day 2 following a right mastectomy with axillary lymph node clearance. She has developed new right axillary swelling, discomfort, and mild shortness of breath, and I’m concerned about a possible early postoperative complication.” B — Background “She has moderate COPD, mild left ventricular failure, and hypertension. Her surgery two days ago was uneventful with 150 mL blood loss, and a drain was inserted. Since yesterday, her temperature has been slowly rising from 36.9 to 37.2 today. Importantly, the drain has had no output today, and the axilla appears swollen and mildly tender. Her daughter is requesting discharge today due to family childcare pressures, but given the clinical changes I feel this is unsafe.” A — Assessment “On examination, she has a swollen right axilla, mild tenderness, and no drain output. Her pain is controlled, and observations are otherwise stable apart from very mild temperature rise. Her bloods today show: WCC 10.2, Hb 11.5, platelets 230. My concern is a postoperative seroma, haematoma, or possibly early infection, or a blocked drain. Given her comorbidities and mild SOB, I also want to rule out cardiopulmonary causes.” R — Recommendation “I’d like you to review her urgently, please. I’d appreciate guidance on whether to: Attempt drainage (needle aspiration) or re-site/flush the drain, Start empirical antibiotics, Arrange ultrasound of the axilla, And confirm whether you agree she should not be discharged today. Could you please come to review her on Ward 4G, or advise on the next immediate steps?” -
MRCS Part B – Communication Station (SBAR Handover)
Time allowed: Reading time: 9 minutes
Interaction time: 9 minutesCandidate Instructions
You are a S.H.O. admitting patients in the Emergency Department.A patient, Ms Jane Doe, a 62-year-old woman, has just arrived with neurological symptoms. The initial assessment and CT head have now been completed. You have reviewed the notes provided.
Your task is to make a telephone call to the on-call Neurosurgical Registrar to hand over the case and request appropriate further management.You must use the SBAR framework to structure your handover.
During the station, the examiner will play the role of the on-call neurosurgical registrar and may ask questions about the case or your clinical reasoning.You should:
Identify yourself clearly at the start of the call.
Provide relevant clinical information succinctly.
Highlight any immediate concerns.
State clearly what you are requesting.
Answer any questions asked.
Demonstrate safe clinical judgement and prioritisation.You should NOT physically examine the examiner or role player.
You should NOT take a history from the patient.At the end of the interaction, close the call appropriately.
Who you are calling
On-call Neurosurgical Registrar
The examiner will play this role.You should assume the neurosurgical registrar is based at the regional neurosurgical centre.
CT imaging is available on PACS for them to review.
Information available to you
Patient notes including initial assessment, observations, drug history, CT result, and ED management (provided on the reading sheet).
You may refer to these notes during the station.
You do not have access to electronic records, except for what is included.
Your Objective
By the end of the call, you should have:
Provided a clear, structured SBAR handover.
Communicated the urgent issues (ICH, high BP, anticoagulation on warfarin).
Requested an urgent neurosurgical review.
Demonstrated awareness of immediate management priorities (BP control, reversal of anticoagulation, level of care).
Shown safe communication, escalation, and closing.
Model answer SpoilerC — SCRIPTED SBAR PHONE CALL (9-minute phone station — candidate lines) (Opening / identification) “Hello, I’m Dr X, a SHO from the Emergency Department. May I ask who I’m speaking to? … I’m calling about a patient called Jane Doe, DOB 15/04/1963, hospital number 0123456 — a 62-year-old lady who arrived 15 minutes ago with a suspected intracerebral haemorrhage. I’d like you to review the patient.” SpoilerS — Situation (short) “She has an acute left basal ganglia intracerebral haemorrhage on CT with intraventricular extension. She arrived 15 minutes ago and is currently in ED resus bay 2.” SpoilerB — Background (brief relevant items) “Key background: Atrial fibrillation on warfarin. Hypertension. Allergies none. On arrival her GCS is 13 (E4 V4 M5), left-sided weakness with power 2/5 in left arm and leg, blood pressure 210/112 mmHg, SpO₂ 97% on air. Point-of-care INR 3.2.” SpoilerA — Assessment (clinical status & investigations) “CT head performed shows a ~3.2 cm left basal ganglia bleed with intraventricular extension; no acute hydrocephalus on initial CT. We’ve given IV labetalol 20 mg once and started oxygen 2 L/min. IV access established, bloods including clotting and group & save sent. She is NBM and being monitored. I’m concerned about ongoing anticoagulation (INR 3.2) and the high blood pressure.” SpoilerR — Recommendation (what you want them to do) “I would like urgent neurosurgical review to assess for surgical intervention/need for transfer. I also recommend immediate reversal of warfarin with PCC and IV vitamin K — could you authorise this or come see? Please advise BP target and agent; if agreeable we plan to target systolic <140 mmHg. Finally, please advise level of care (HDU/ITU) and whether you want a CT repeat and timing. I can send you the CT images to review on PACS and have the patient ready for review now in resus bay 2 — can you come to ED or should we arrange transfer?” Close “Thank you — I’m able to give you further information or bring the patient to the neurosurgical unit if advised. My contact is bleep 321. Do you need any additional details now?” D — Examiner / Marking tips & likely questions to expect Key points examiners look for (communication and clinical content): Clear identification and succinct SBAR structure. Immediate recognition of reversible causes and time-sensitive actions: urgent reversal of warfarin (PCC + vitamin K) and BP control. Clear request for neurosurgical review and suggestion of level of care (HDU/ITU). Safe airway plan (NBM, prepare for decline), monitoring plan and clear escalation triggers. Appropriate documentation: CT findings, GCS, observations, anticoagulant status and INR. Likely follow-up questions the examiner/onsite consultant may ask (prepare short answers): “What is the exact CT finding?” → Left basal ganglia ICH ~3.2 cm with intraventricular extension; no acute hydrocephalus. “What’s her INR and when was last warfarin dose?” → INR 3.2 (POC); husband reports she took warfarin that morning. “What have you given already?” → IV labetalol 20 mg once; oxygen; analgesia; IV access; bloods sent. “What BP target do you propose?” → Target systolic 130–140 mmHg if tolerated; recommend nicardipine infusion if boluses fail. “Is she a surgical candidate?” → Unsure — needs neurosurgical assessment; size and intraventricular extension raise concern; recommend urgent neurosurgical review for EVD/consider decompression/transfer. Pitfalls to avoid in the station Missing anticoagulation status. Forgetting to ask for neurosurgery. Not naming a BP target or asking for specific reversal agents. Failing to document GCS or a change in GCS as an escalation trigger. -
Stem:
You are the surgical SHO on call. Mrs. Janice Green, a 54-year-old woman, has been complaining of chronic back pain. She has asked you to help her in your FY1 colleague, and an MRI was performed previously. The consultant has asked you to go in and take a focused history from her to narrow down the cause.
Please take a history from the patient. You do not need to perform a physical examination. At the end of the consultation, you should try to explain and ask you to summarize your findings and ask you questions about the case.
Examiner: Please summarize your case. "Mrs Janice Green is a 54-year-old woman with 4 months of chronic lower back pain, dull and aching, sometimes shooting down both legs to her feet, increasing in intensity, keeping her awake at night, worsening. She denies numbness, weakness, or bladder/bowel problems. She has hypertension, is unemployed, and she primary carer for her disabled husband, reporting significant stress and functional limitation. She has had a previous MRI, and no other systemic symptoms. This is most likely mechanical back pain, but red flags include night pain and possible weight loss, so further evaluation and broad support are appropriate." Examiner: How would you manage this patient? I would inform my seniors, perform a clinical examination, and order some investigations including: Full blood count: Looking for anemia which may indicate malignancy, leukocytosis which may indicate infection or inflammatory causes. Serology: Which may indicate an autoimmune process such as rheumatoid arthritis. Plasma electrophoresis: For possibility of multiple myeloma. Liver function tests: For possibility of metastatic disease or as part of an extraintestinal manifestation of inflammatory bowel disease. Plasma amino-lipase: May be considered if pancreatitis is suspected. Urea and electrolytes: May be ordered especially if the suspected diagnosis is multiple myeloma, which is associated with renal failure. Radiological investigation may include: X ray of the spine: Looking for bony abnormalities. MRI of the spine: Looking for disc pathology, spinal cord/cauda equina compression, or to determine diagnosis such as facet joint arthropathy. Abdominal ultrasound scan: if an abdominal aortic aneurysm is suspected. CT scan of the abdomen: may be considered if a diagnosis of chronic pancreatitis is suspected. Treatment will be tailored to the underlying cause, in this case the likely cause is primary or secondary spine malignancy, it needs to be discussed in a MDT meeting, if disseminated malignancy it will likely include radiotherapy, chemotherapy, and pain management, if her pain is complex pain management teams may be included. Note: When formulating a management plan, inform the patient, it is not mandatory that you get the right diagnosis, just give a reasonable set of investigations that will help you reach the diagnosis, and treatment plan for the most likely diagnosis in a brief manner. Note: When formulating a management plan, always remember that you are NOT ALONE, always involve other parts of the team, for example, pain management team, radiologist, pharmacist... etc. according to the case you are dealing with. -
You are the surgical SHO in clinic.
Mr. David Johnson,
a 50-year-old former
semi-professional football player,
presents with right knee pain
For the last 4 months.
He underwent surgery on the same knee
30 years ago following a football injury,
but does not recall the exact details
of the procedure.You are not required to perform clinical examination.
Please take a focused history
to assess the cause of his current knee pain.
Discussion Examiner: Summarize your case and give a differential "Mr. David Johnson is a 50-year-old former football player with a background history of Diabetes mellitus on Metformin, who presents with 4 months of right knee pain. The pain is gradual in onset, dull and aching, worsens with activity and at the end of the day, and improves with rest. He reports morning stiffness of about 10 minutes. He had a knee injury and surgery 30 years ago, details of which are unclear. There are no associated swelling, redness, systemic symptoms, or other joint involvement." The most likely diagnosis is post-traumatic osteoarthritis on the account of his past knee injury, his pain also being in keeping with the differentiating and exacerbating include: Chronic meniscal tear. Inflammatory arthritis such as ankylosing spondylitis or rheumatoid arthritis. Primary or secondary bone malignancy. Osteonecrosis of the knee. Crystal arthropathy including gout and pseudogout. Septic arthritis, which is unlikely. Give your main diagnosis, and then list the others, try to make a list from the most likely to the less likely. Examiner: What is your management plan? I would first examine the patient, and inform my seniors to get their advice, this will allow me to order a more focused set of investigations, but investigations needed may include: Biochemical investigations: FBC: Looking for anemia, which is seen with malignancy, chronic disease, and inflammatory bowel disease, leukocytosis, which is seen with infective or inflammatory pathologies. CRP and ESR: As inflammatory markers. Serology: looking for autoimmune process is suspected such as rheumatoid arthritis. Imaging: X-ray of the knee in two views looking for signs of osteoarthritis. MRI scan of the knee which can better characterize osteoarthritis, detect early changes, and detect meniscal or ligamentous injuries. Examiner: How would you treat this case? After discussion with my seniors, treatment will be tailored to the underlying diagnosis, in this case osteoarthritis is most likely, treatment options can include: Conservative treatment: Achieve healthy weight and maintain exercise, this will reduce mechanical stress on the joint. Physiotherapy, focusing on strengthening the muscles around the knee. Analgesia, this may include paracetamol or NSAID's. Intra-articular steroid injections. Surgical management: Total or partial arthroplasty. Arthroscopy, in conclusion if there are loose bodies or meniscal tears, but it does not affect the progression of osteoarthritis. Realignment osteotomies, which are designed to redistribute weight away from the affected knee compartment, it can delay the need for arthoplasty. Examiner: If total knee replacement is carried out, what are the causes failure of total knee replacement? Aseptic loosening of the implant. Wear and tear in the joint. Early or late prosthetic joint infection. Periprosthetic fractures. Examiner: What do you mean by aseptic loosening? Aseptic loosening refers to the separation of the implant from the bone due to chronic inflammatory reaction, it does not involve bacterial infection, rather the debris from the wearing of implant components triggers an inflammatory reaction in the surrounding bone, leading to osteolysis, bone loss and implant loosening over time, it is a long term complication. Examiner: Will this patient be able to play soccer in 9 months after a total knee replacement, and why? Unlikely to be able to play soccer in 9 months, it is generally not recommended because this can damage the prosthesis and cause early loosening of the implant. Examiner: What X ray findings are consistent with osteoarthritis? Joint Space Narrowing (JSN) -
Lateral
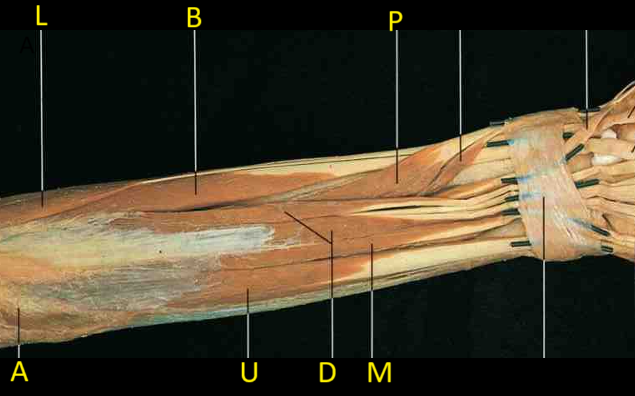
MedialExtensor Carpi Radius Longus.
Extensor Carpi Radius Brevis.
Abductor Pollicis Longus.
Anconeus.
Extensor Carpi Ulnaris.
Extensor Digitorum.
Extensor Digiti Minimi.
Left hand from behind [image: 1760103624953-9f4ae09c-23ed-4f41-907e-e8b42e8dac62-image.png] 11 Extensor pollicis brevis. 12 Extensor pollicis longus. 6 Extensor carpi radialis longus. [image: 1760103624953-9f4ae09c-23ed-4f41-907e-e8b42e8dac62-image.png] 5 Extensor carpi radialis brevis. 9 Extensor digitorum 10 Extensor indicis [image: 1760103624953-9f4ae09c-23ed-4f41-907e-e8b42e8dac62-image.png] 8 Extensor digiti minimi 14 First dorsal interosseous 16 Second dorsal interosseous answers[image: 1760103639333-44029a07-c8b5-4502-b891-25e7ee396749-image.png] -
Anterior [image: 1757607222780-090205a8-dc19-4036-baa6-c265e07a8591-image.png] Spoiler [image: 1757606977748-a7046645-fb1e-41d8-9a6a-60a411ec8218-image.png] Posterior [image: 1757606627233-8bb534ad-b401-4a07-8b0c-8ee290285be8-image.png] Spoiler[image: 1757606789866-c65988de-927e-49f3-a303-5fab5b16c349-image.png] -
Station Topic: Brain Anatomy – Internal Carotid Artery Question (20 marks) [image: 1759597375048-2ab79662-441a-40de-b185-1c9d05240885-image.png] You are asked to demonstrate your knowledge of the internal carotid artery (ICA) and its relation to brain anatomy. Identify and describe the course of the internal carotid artery from the neck to the brain. (5 marks) Spoiler1 The ICA arises from the common carotid artery at the level of C3–C4 vertebrae. Cervical segment: Ascends vertically in the neck without branching. Petrous segment: Enters the carotid canal in the petrous temporal bone; runs anteromedially. Cavernous segment: Courses through the cavernous sinus; forms an S-shaped curve (the carotid siphon). Cerebral (supraclinoid) segment: Exits the cavernous sinus and pierces the dura mater at the roof of the cavernous sinus to enter the subarachnoid space; gives terminal branches to the brain. Tip: Remember mnemonic “Cervical, Petrous, Cavernous, Cerebral” to recall ICA segments. 2 List and explain the main branches of the internal carotid artery in the cranial cavity. (5 marks) SpoilerOphthalmic artery: First branch; supplies the orbit and optic nerve. Posterior communicating artery (PComm): Connects ICA to posterior cerebral artery; part of Circle of Willis. Anterior choroidal artery: Supplies choroid plexus, internal capsule, optic tract. Terminal branches: Anterior cerebral artery (ACA): Medial frontal and parietal lobes. Middle cerebral artery (MCA): Lateral convexity of cerebral hemisphere. Tip: ACA + MCA = terminal branches; remember PComm is part of collateral circulation. 3 Describe the areas of the brain supplied by these branches. (5 marks) SpoilerBranch Area Supplied Ophthalmic Eye, orbit, optic nerve Posterior communicating Connects ICA to posterior cerebral artery; collateral supply to occipital lobe Anterior choroidal Posterior limb of internal capsule, optic tract, globus pallidus, choroid plexus Anterior cerebral (ACA) Medial frontal and parietal lobes; leg motor/sensory cortex Middle cerebral (MCA) Lateral convexity of hemisphere; face and upper limb motor/sensory cortex, Broca/Wernicke areas Clinical Relevance of ICA (5 marks) Outline the clinical relevance of the internal carotid artery. Include at least two common pathologies and their implications. SpoilerAtherosclerosis / ICA stenosis: Can cause transient ischaemic attacks (TIAs) or stroke in MCA/ACA territories. Risk factors: hypertension, diabetes, smoking. Aneurysm formation: Common at bifurcation into MCA and ACA or posterior communicating artery. May cause subarachnoid haemorrhage or cranial nerve III palsy if PComm involved. Other considerations: SpoilerICA injury during carotid endarterectomy. Compression by tumours (e.g., pituitary adenoma in cavernous sinus) → ophthalmoplegia. -
Humerus A) Front C) Medial

Greater tubercle.
Lesser tubercle.
Surgical neck.

Head.
Intertubercular groove.
Anatomical neck.

Lateral and Medial lip of intertubercular groove.

Deltoid tuberosity
Right humerus lower end, A) Front B) Behind [image: 1760100719273-504353c4-52fc-4100-b8c5-d7b78397d7f0-image.png] 2 Capitulum. 5 Lateral epicondyle. 13 Trochlea. [image: 1760100719273-504353c4-52fc-4100-b8c5-d7b78397d7f0-image.png] 7 Medial epicondyle. 8 Medial supracondyle ridge 10 Olecranon fossa. -
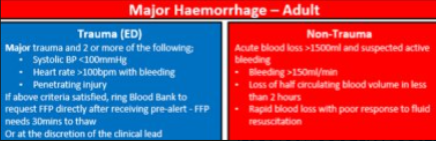
A 35-year-old male is brought to the emergency department after a high-speed road traffic accident. He is pale, clammy, hypotensive (BP 80/50), tachycardic (HR 130), and confused. There is obvious major bleeding from a laceration to his thigh.You are asked to manage this patient according to the Major Haemorrhage Protocol (MHP).
- What is Initial Assessment and Immediate Actions (6 marks)
-

1 Where do the secretions of the parotid gland drain?The secretions of the parotid gland pass into the oral cavity via Stensons duct whose oral opening is opposite the second upper molar tooth.
2 Which structures pass through the parotid gland?
Facial nerve
External carotid artery
Retromandibular vein
Auriculotemporal nerve3 What is the lymphatic drainage of the parotid gland?
It contains lymph nodes within the substance of the gland itself. It then drains to the deep cervical nodes.
4 Which nerves supply the parotid gland?
Parasympathetic-Secretomotor
Sympathetic-Superior cervical ganglion
Sensory- Greater auricular nerve5 Outline where you would place the incision for a superficial parotidectomy.
The incision runs posterior to the mandible and up inferior to the tragus of the ear. Loss of cutaneous sensation to the ear lobe is therefore a risk of the procedure.

read more →@admin said in Station - parotid gland: Parasympathetic Parasympathetic (secretomotor) innervation The parasympathetic supply increases the production of watery saliva. Its pathway is long and complex, beginning with the glossopharyngeal nerve (CN IX). Origin: The preganglionic parasympathetic fibers arise from the inferior salivatory nucleus in the brainstem. Course: The fibers travel along the glossopharyngeal nerve and a small branch called the tympanic nerve, which passes through the middle ear. Synapse: The fibers continue as the lesser petrosal nerve and synapse in the otic ganglion, which is a collection of nerve cell bodies near the base of the skull. Supply: The postganglionic fibers then "hitchhike" along the auriculotemporal nerve (a branch of the trigeminal nerve) to reach and innervate the parotid gland. (Hence sometimes post parotidectomy when the great auricular nerve is sacrified or injured - it causes Frey's syndrome - where regenerating of parasympathetic fibers accidentally "rewire" themselves to connect with the sympathetic pathways that lead to the skin's sweat glands and blood vessels Sympathetic innervation The sympathetic supply reduces saliva production, causing a thicker, more viscous saliva via vasoconstriction. • The postganglionic sympathetic fibers originate from the superior cervical ganglion and travel to the gland along the external carotid artery. Sensory innervation The parotid gland receives its sensory supply from two nerves. • Auriculotemporal nerve: This nerve provides general sensory innervation directly to the substance of the gland. • Great auricular nerve: This nerve, a branch of the cervical plexus (C2 and C3), supplies the sensory innervation to the tough fascia or capsule of the parotid gland.

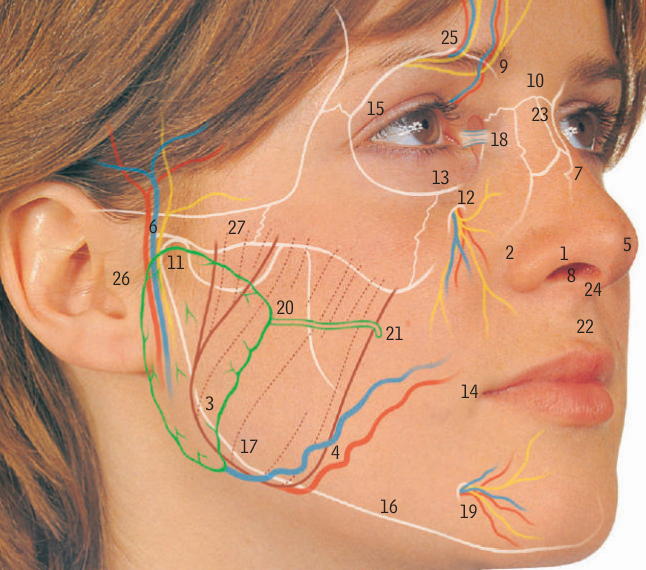


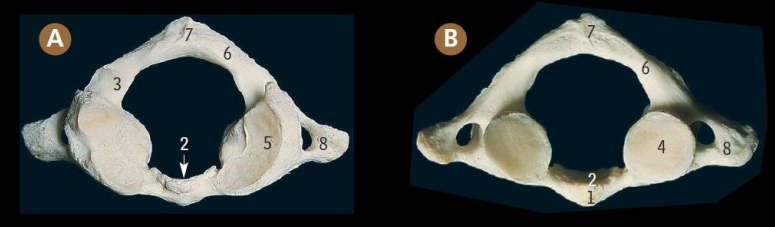
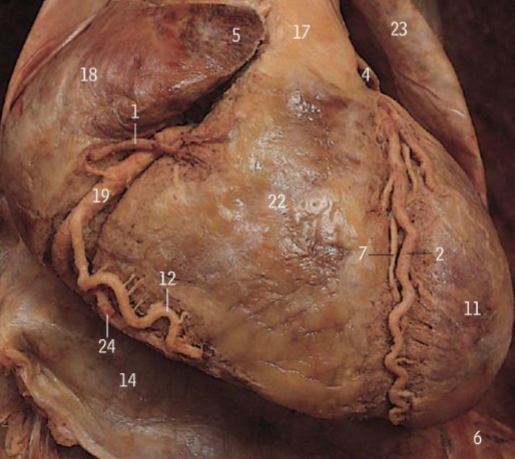
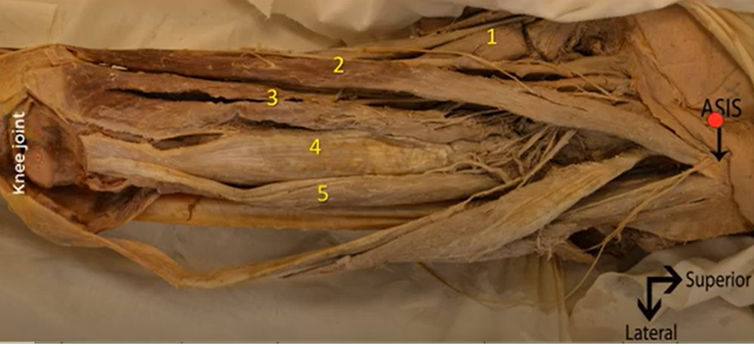
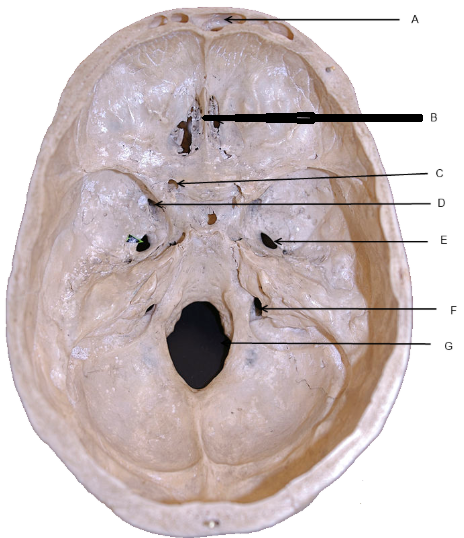
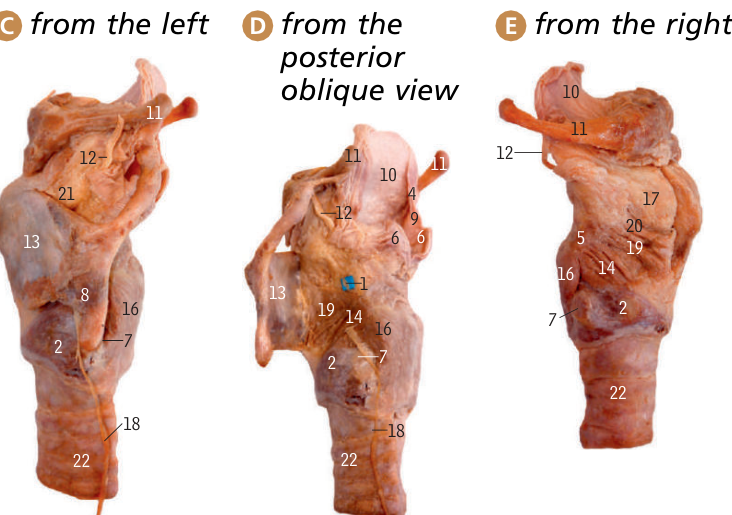
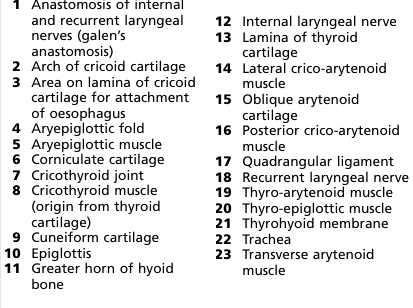
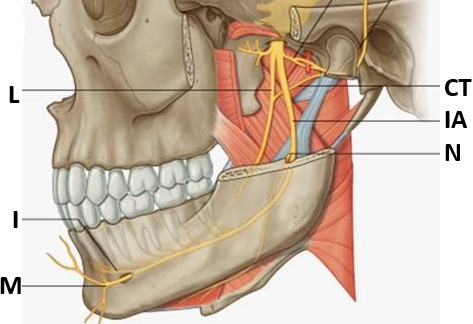
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}