further notes on https://mrcsrevisionnotes.wordpress.com/
A
admin
@admin
Posts
-
drive link -
drive link -
PRE-OPERATIVE ASSESSMENTPRE-OPERATIVE ASSESSMENT BEFORE THR
STEM - A 62-year-old man came for his preoperative assessment in Orthopaedic OPD for his scheduled THR in one week, He was diagnosed with OA & months ago, and his operation was cancelled due to his reluctance. Now, his wife has managed him and taken him to Orthopaedic OPD to get a schedule soon as they are going to arrange their daughter's wedding in 2 weeks.
Now that you are an orthopaedic SHO, considering this a history-taking station, go through his preoperative assessment to inform your consultant.(This station is deviated largely from the usual history format. Here patient is already diagnosed and has done all the relevant investigations and came to SOPD to get his schedule for THR with his wife who actually convinced him for operation. There's no need to ask about pain, similarly no need ask questions for differentials. This station largely focuses on pre-operative fitness status, co-morbidities, medications, PMH, PSH that are most concerned issues before operation which need to be optimized).
- Introduce yourself
- Hello, good morning, I’m Dr. Z, one of your surgical doctors.
- Confirm patient's ID and verbal consent
- = Just for documentation purposes, could you please confirm me your name and age please?
- = Nice to meet you! Good to see you again Mr. X.
- =I do believe that today you are here to get schedule for your upcoming hip surgery. Before that, I've been told to ask you few questions regarding your health condition and to assess how fit you are for your surgery and anaesthesia so that we can take appropriate measure accordingly. Are you okay with that?
- Assess respective concern
- Mr. X, how’re you feeling today? Is your leg hurting much?
- I'm so sorry to hear that. I understand you are passing through a difficult situation right now.
- Past medical history & medication history
- May I know, Mr. X, whether you have been diagnosed with some medical conditions or not? Do you have any chronic illness?
(The patient will bring his prescription and drug list & will tell you to check this. Don't take it; instead, assure him you will check his file once your conversation is finished).
(Now ask elaborately about those conditions that the patient says one by one)-
Diabetes
-
How long has it been? Is it under control?
-
Which medication do you take? Dose? How long?
-
Do you have any problems with your feet and hand? Any numbness?
-
Anything wrong with your Vision?
-
Asthma / COPD
-
How long has it been? Is it under control?
-
Which medication do you take? Dose? How long? (ask specially for steroids and inhalers)
-
Cardiac issues, Hypertension
-
How long has it been? Is your HTN under control?
-
Which medication do you take? Dose? How long?
-
Do you have any issues with your heart?
-
Are you attending your cardiology doctor and warfarin clinic regularly?
5. Past surgical history
- Have you undergone any surgeries before? (H/O CABG 2 years back, pacemaker insertion 4+ years ago, left nephrectomy 7 years ago)
- Was there any problem with surgeries or anaesthesia? If yes, what was that?
- Personal history
- Who do you live with?
- Do you smoke? If yes, how many cigarettes & how long?
- Do you take alcohol? If yes, how many units & how long?
- General fitness & systemic review
-
How far can you walk normally before breathlessness stops you?
-
Is it for pain or are there any other issues?
-
Do you take physiotherapy?
-
Ask for constitutional questions as part of systemic review.
-
Now patient may ask you some questions, for example, “Doctor, when will | be scheduled for my hip surgery? My daughter's wedding is in 2 weeks, Please get me scheduled.as soon as possible”.
-
Your answer would be, “Mr. X. I completely appreciate your concern. Please pardon me, but I can’t tell you my thoughts right now, As you have several medical & surgical conditions and you're on various medications, to ensure a safe surgery and safe anaesthesia for you, we must optimize your health condition and medications first.
Considering these, I think you're not fit for this major surgery at this moment. Mr. X, I assure you that I will discuss about your surgery with my consultant as soon as possible,
We need to discuss and seek opinions from endocrinologists, pulmonologists, cardiologists, physiotherapists, and urologists (depending on the history) about optimizing your health condition before surgery. Only after the opinion from MDT, we can schedule the date for your hip surgery.”
PRESENTATION
Mr. X, a 62-year-old man, came to SOPD for the awaiting THR. On preoperative assessment, he is noted to have DM/HTN/COPD/CAD. He has a past surgical history of CAG and pacemaker insertion 2 years back, CABG 4 years back and right nephrectomy 4 years back. In addition, he is commenced on warfarin and oral prednisolone,
Considering his past medical and surgical history, he is not fit for surgery this week as he needs an opinion from MDT, and his warfarin and steroid which need to be optimized along with his comorbidities.
Is the patient fit for surgery? Why do you think like that?
I don’t think Mr. X is fit for surgery and anaesthesia. Because of having Significant cardiac history (CABG, Pacemaker)
HTN
COPD
Diabetes
Patient is on warfarin that must be bridged
Patient is on steroids which should be optimized to prevent Addisonian crisisWhat are your differentials for hip pain at this age?
I would consider
OA
RA
AVN
Paget's disease of bone
Neoplasm
Septic arthritisHow will you optimize his conditions before operation? What are your considerations pre-operatively for this patient?
I will discuss with MDT- Diabetes control (see OR listing station)
HTN control with opinion from cardiologist
Pre-op pacemaker setup control (sce OR listing station)
Reversal of warfarin (see OR listing station)
Asthma’ COPD optimization (see OR listing station)
Steroid optimization (see ASSCC steroid station)
Optimize pre-op fluid and electrolyte imbalance as he has only one kidney
Pre- and post-operatively under supervision of physiotherapist
Pre-op thromboembolic prophylaxis (risk factors include orthopaedic operation, patient may have
polycythemia due to COPD)
-
Dysphagia historyHistory Taking Station: Dysphagia
Station length: 7–9 minutes
Task: Take a focused history from a patient presenting with difficulty swallowing.Candidate Instructions
You are the surgical trainee in clinic.
A patient has been referred with difficulty swallowing (dysphagia).
Please take a focused history and summarise your findings to the examiner.Examiner Mark Scheme
Total marks: 20-
Introduction and Communication (2 marks)
Criterion Marks
Introduces self and role 1
Confirms patient identity and explains purpose of consultation 1 -
Presenting Complaint (2 marks)
Criterion Marks
Clarifies the nature of the swallowing difficulty 1
Establishes duration and onset of symptoms 1 -
Characterisation of Dysphagia (4 marks)
Criterion Marks
Differentiates solids vs liquids 2
Establishes progression of symptoms 2
Key diagnostic points expected:
Difficulty with solids progressing to liquids
Whether symptoms are progressive or intermittent -
Associated Symptoms (4 marks)
Criterion Marks
Weight loss 1
Regurgitation of food 1
Pain on swallowing (odynophagia) 1
Persistent vomiting or choking episodes 1 -
Red Flag Symptoms (3 marks)
Criterion Marks
Unintentional weight loss 1
Vomiting or haematemesis 1
Progressive worsening dysphagia 1 -
Gastro-oesophageal Symptoms (2 marks)
Criterion Marks
Heartburn / reflux symptoms 1
History of long-standing reflux disease 1 -
Risk Factors (2 marks)
Criterion Marks
Smoking history 1
Alcohol intake 1 -
Medical and Drug History (2 marks)
Criterion Marks
Relevant past medical history 1
Drug history including NSAIDs or medications affecting oesophagus 1 -
Summary and Clinical Reasoning (3 marks)
Criterion Marks
Provides structured summary 2
Identifies concerning features suggesting malignancy 1
Example expected summary:
"A middle-aged patient with progressive dysphagia to solids associated with weight loss, raising concern for an oesophageal malignancy."Candidates should demonstrate the ability to:
Structure a focused surgical history
Identify red flag features of upper GI malignancy
Differentiate mechanical obstruction vs motility disorder
Communicate clearly and summarise effectivelyCommon Candidate Errors
Failure to ask about progression of dysphagia- Not asking about weight loss
Forgetting smoking and alcohol history
Not summarising the case at the end -
-
SpotterApp -
Appendix + Abdo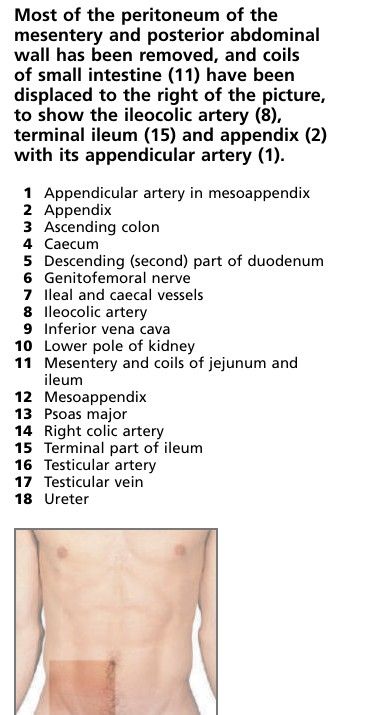
-
Appendix + Abdo
-
Anxious motherANXIOUS MOTHER (PERFORATED APPENDIX)
STEM - You are a surgical SHO on call for emergency general surgical admissions. A 10-year-old girl Sarah was brought by her neighbour as an emergency with peritonitis, Her mother was at work when she was told that her daughter is in hospital.
The child Sarah, is febrile and extremely ill, A perforated appendix is suspected and she is being resuscitated by your registrar before being taken to the operating theatre. You've just arrived in the hospital for your shift and haven't seen the patient. Your consultant, Mr, Mann is on his way from home, and will perform the operation, She became anxious when she realize that Mr. Mann is the same surgeon who operated upon her husband and couldn't save his life.
Considering this communication skills station, you are asked to talk to this anxious mother and answer her queries.
Doctor: Hello, good evening, I'm Dr. Z, one of the surgical doctors. Am I talking to Sarah's mother? *Patient: It's not a good evening for me, doctor, at all. What's going on here? All of you have taken my child for an operation even without letting me know. How is this even possible?* Doctor: I was told to speak with you about your child condition. Can we please have a seat so that we can discuss about everything a bit more detailed? Could you first tell me what do you know so far? *Patient: My child had fever from yesterday; but still I went to my work. I have no clue, doctor. It's all happened because of not being in home.* Doctor: First, you don't have to feel guilty because this could happen anyway. Your daughter was brought by your neighbour complaining of tummy pain. Our initial investigation revealed the suspicion of acute appendicitis. She was managed by our registrar and received some TV fluids and antibiotics. We are now waiting for theconsultant who will operate upon her. *Patient Are you sure that my daughter has acute appendicitis?* Doctor: We are suspecting acute appendicitis as this is common condition and also her signs and symptoms denotes this. But we cannot be certain 100% until we open and see. Usually we do a keyhole first, then look for it. Then after observation we complete the procedure. if it ruptures and case general infection of your tummy, or if this failed, we need to convert it to open appendectomy by giving a small incision over right lower tummy. *Patient: Is it dangerous, doctor?* Doctor: In children specifically, there is less fat inside the abdomen, so perforation can be particularly dangerous. In such case your child may go to a higher care area called HDU. But Mr. Mann is a very good surgeon, I can assure you that your childis in very good hands. We will be looking after her but there are still some concerns. *Patient: Will the wound be disfiguring?* Doctor: A small horizontal wound will leave a little scar, but we may need to expand the wound and this may leave a bigger scar. We will try to make as little scar as possible. / As she is a girl, it's conecrning, but still we will try to make it as short as possible. *Patient: Is there any other problem that could occur?* Doctor: Yes, probably severe infection can block the reproductive tubes in young girls, so future sub fertility may happen. *Patient: Do you mean that she can’t get pregnant in the future?* Doctor: I understand your apprehension, no need to worry because she has another fine working tube on the other side. *Patient But Mr, Mann did operation for my husband, and he died,* Doctor: I am so sorry to hear that. Please accept my sincere condolences. May I ask when and how he died? *Patient: Mr. Mann did operation for him because he had colon cancer and he died few weeks after the operation at home.* Doctor I am so sorry to hear that again. I think those are two different situations. I think your husband died from the cancer not the surgery and Mr. Mann one of best surgeon we have in the hospital who has a vast experience on this, we will take good care of your daughter. *Patient: Can I change the consultant?* Doctor: Of course, you can because it's within your rights. But it’s time consuming as the new consultant will study the case from the beginning. As i's a suirgical emergency it will have a deleterious impact on your child health. So, I will not recommend you do that. *Patient: Can I see her?* Doctor: Obviously, you can see her. But she will be kept in observational room just after the operation. Once she regains her consciousness, you can definitely see her. Do you have any other concerns? *Patient: I just need to be everything ok for my child.* Doctor: Of course, my team is trying our best. Lets summarize what we have been through here. Your child has been brought here by your neighbour complaining of tummy pain. Our initial investigation revealed acute appendicitis and we are now waiting for the consultant to operate upon her, and I’ve explained the risks and benefits of this operation. We all are here to help and support you and to dive you a hand at any time. Should there be any concerns, please don’t hesitate to contact me at any moment. I will leave my bleep number at the nurse station. Thank you so much for your co-operation. -
isb11 Face surface markings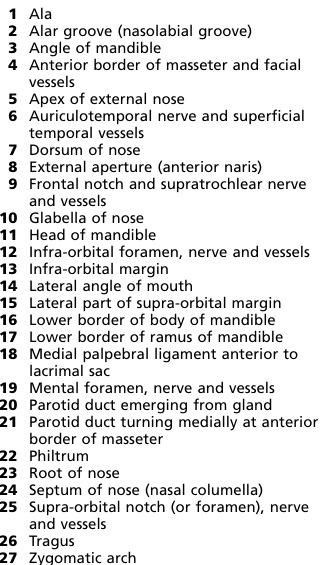
-
isb11 Face surface markings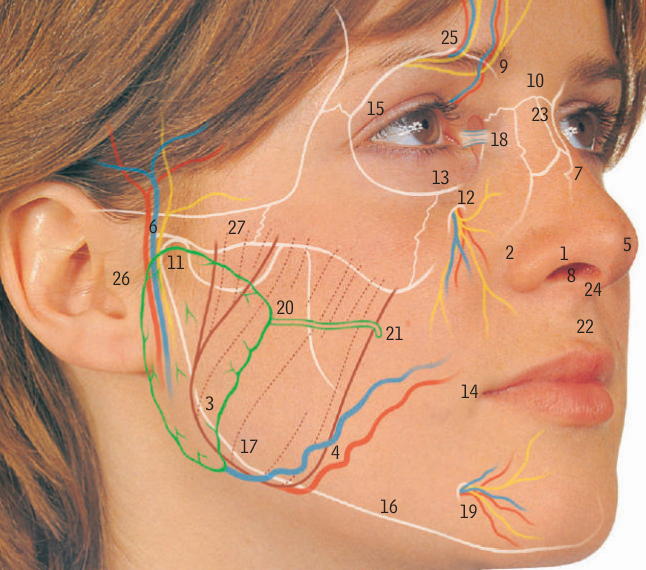
-
isb2 Neck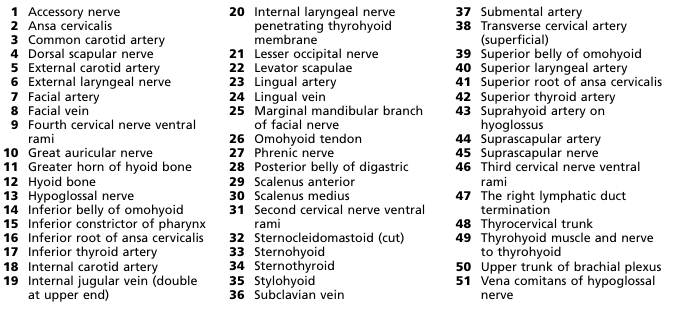
-
isb2 Neck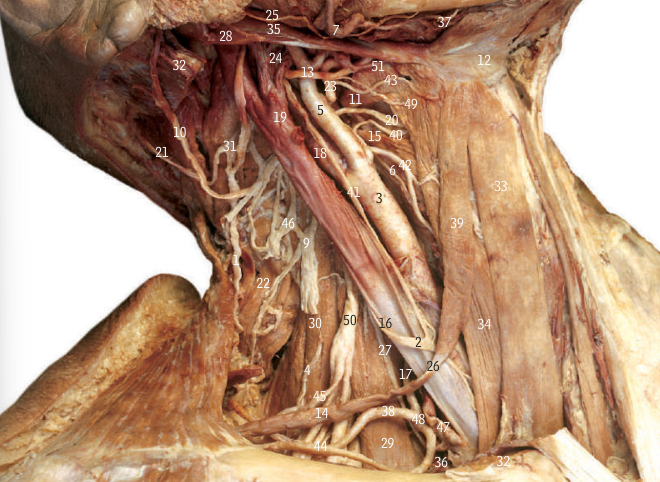
-
Post-Op reactive depressionPRESENTATION
John, a 56-year-old occupation, previously fit/smoker/social drinker who is on his 5th POD following ... [e.g. right hemicolectomy], has showed signs of anhedonia, depression and fatigue. He has also showed some signs of positive core biological symptoms.
Considering all of this, my provisional diagnosis is reactive (postoperative depression), I will also consider major
depressive disorder, bipolar disorder.What will be your management?
For mild conditionRegular exercise
Advice on sleep hygiene (regular sleep times, appropriate environment)
= Psychosocial therapy -CBT
Moderate to severeRegular exercise, advice on sleep hygiene
CBT
Medication -SSRIs
High-intensity psychosocial intervention (CBT or interpersonal therapy)
Immediate and considerable high risk to themselves or others: Admit to psychiatric ward (use Mental Health
Act if necessary) -
Post-Op reactive depression- Introduce yourself
Hello, good morning, I’m Dr. X, one of the surgical doctors today. How are you doing today?In this station, the patient is hospitalized and is now in postoperative period. So, you will not ask for name or age or Past medical or surgical history, Drug history, Family history, Ideas, concerns and expectations, other system review. |
- Obtain verbal consent
Would you mind if ask you some questions regarding your conditions?- Main history - [Divided into_3 segments that you have to assess; Core symptoms of depression, biological
symptoms of depression, past psychiatric history |
A. Core symptoms of depression (depression, anhedonia and fatigue)
* In the past days during your hospital stay * Have you felt down, depressed or hopeless? (Depression) * Found that you no longer enjoy, or find little pleasure in life? (Anhedonia) * Been feeling overly tired? (Fatigue)B. Biological symptoms of depression (mnemonic SMALL)
SleepHow has your sleep pattern been recently? Have you had any difficulties in getting to sleep? Do you find you wake up early, and find it difficult to get back to sleep?Mood
Are there any particular times of day that you notice your mood is worse? Does your mood vary throughout the day? Do you find that your mood gradually worsens throughout the day?Appetite
Have you noticed a change in your appetite? What is your diet like at the moment? What are you eating on a typical day?Libido (Seek permission again — I'm asking you some personal questions that include about your sexual life, and it would help me to reach a diagnosis and help you out. Whatever the information you give me, it will remain
confidential between us. Are you okay with this?)* Have you noticed any change in your libido? * Since you have been feeling this way, have you noticed a difference in your sex drive?C. Past psychiatric history - Previous episodes of depression or dysthymia
Have you ever felt like this before? Have you ever had any other periods of feeling particularly low? In the past, have you had any problems with your mental health? Have you had any counselling for any issues before? Have you ever been admitted to hospital because of your mental health? If so, obtain details -time, method of admission, result.POSITIVE FINDING
Positive core and biological symptoms of depression. -
Post-Op reactive depressionSTEM 1 - You are asked to take the history John, a middle-aged male on the 5th post-op day who has presented with low mood for 6 hours and loss of appetite. He is not willing to talk to anyone and seems to be lost, The nursing staff informs you that he has been sleeping poorly post-operatively.
-
NeuroSurgSpinal Stenosis
Doctor Instruction:
Your next patient is a 51-year-old woman called Rebecca, presenting with lower back pain. Please take a history and perform an appropriate examination.
Patient History:
Rebecca, a 51-year-old female, nurse
You have always been having lower back pain for the past few years, but this has been getting gradually worse. The pain is dull and intermittent. Very often, the pain can diffuse and radiate towards the buttocks, back of the thighs, and feet - when this happens, the pain feels like a burning or cramping sensation. It can be associated with weakness in both legs. The symptoms can be triggered or worsened by sitting down, standing straight and walking downhill. It goes away after a few minutes after being at rest. Bending forward improves symptoms. You tried paracetamol, which only helped a little with pain.
If you walk for more than 50 yards, you will start noticing numbness and weakness in your legs.
No previous injury/trauma. Waterworks normal. The bowels are working normally. No other abnormal sensations or weaknesses. No incontinence. No stiffness. No fever. No weight loss. No night sweats.
Ideas, Concerns, Expectations:
You think because you often have to bend your back due to work, the pain may be caused by poor posture. You are concerned because it is starting to affect your ability to work in the hospital as a nurse. You would like to see if you can get stronger painkillers and possibly have a scan of your back.
Past Medical History:
Obesity, hypercholesterolemia, acromegaly, T2DM.
No past relevant surgical history.
Drug History:
Atorvastatin, metformin NKDA.
Family History:
Father has ankylosing spondylitis.
Social History:
You work as a senior nurse in a local hospital.
You smoke around ten cigarettes daily for over ten years but don't drink alcohol.
Live with husband in a semi-detached house.
Independent.
Examination Findings:
Lower spinal tenderness on palpation at L4-5 region.
Complete motor and sensory neurological examinations are normal.
Features of acromegaly e.g. enlarged hands, feet and facial features.
Lower limb vascular examination is normal.
No cervical tenderness or restricted movement. Gait normal.
No cauda equina syndrome features.
Peripheral pulses and ABPI normal.
Differentials:
Lumbar spinal stenosis - likely to be due to degenerative changes
Osteoarthritis of the spine
To rule out cauda equina syndrome
Ankylosing spondylitis/spondylolisthesis
Rule out peripheral arterial diseases
Other causes of back pain: spinal tumour, disc herniation, trauma, fracture, and epidural abscess.
Investigations:
Imaging:
XR Lumbar spine (may show degenerative changes/spondylolisthesis)
MRI Spine. Alternatively, CT myelography/spine when MRI is not available or unsuitable.
Consider ABPI / CT angiogram to exclude peripheral arterial disease where intermittent claudications are present.
Special tests:
Consider electromyographic (EMG) walking test - increased F latency values in lumbar spinal stenosis
Consider electromyographic paraspinal mapping
Management:
Conservative:
Exercise
Weight loss if overweight
Physiotherapy e.g. exercises that minimally stress the back, such as walking, swimming, or bicycling. Exercise may also strengthen the paraspinal muscles.
NSAIDSs e.g. naproxen, celecoxib +/- PPI cover / antacids
Paracetamol
Medication for neuropathic pain e.g. amitriptyline, gabapentin, pregabalin.
Consider oral steroids for acute exacerbation of painful symptoms.
Activity modification e.g. limit heavy lifting/prolonged sitting/repetitive bending/twisting of the back.
Consider deep heat therapy with massage to relieve spasms associated with back pain
Surgical:
Consider decompression surgery +/- fusion e.g. laminectomy ( removal of the lamina from affected vertebra) followed by physiotherapy
Consider interspinous distraction procedure to reduce backward movement of the spine.
Consider epidural injections with local anaesthetic and corticosteroids under specialist guidance for short/long-term pain relief.
Viva Questions:
Explain the pathophysiology of spinal stenosis.
Spinal stenosis is the narrowing of the spinal canal, which holds the spinal cord and nerves. It's often due to age-related disc degeneration, arthritis, and thickened ligaments. This narrowing can compress the spinal cord and nerves, leading to pain, numbness, and weakness. Factors like herniated discs and inflammation worsen the compression. Treatment involves pain management, physical therapy, and sometimes surgery to relieve pressure on the nerves and spinal cord.
At what level of the spine does spinal stenosis occur most commonly?
Spinal stenosis most commonly occurs in the lumbar (lower back) region of the spine. This is because the lumbar spine bears the most weight and undergoes significant movement, which can contribute to degenerative changes over time. Lumbar spinal stenosis can result in compression of the spinal cord and nerve roots, leading to symptoms such as lower back pain, leg pain, numbness, and weakness. However, spinal stenosis can also occur in the cervical (neck) and thoracic (mid-back) regions of the spine, albeit less frequently.
What are the causes of spinal stenosis?
Degeneration of spinal structures due to aging.
Disc degeneration and herniation.
Osteoarthritis and bone spurs.
Thickened ligaments.
Congenital factors and genetics.
Injuries and trauma.
Tumors or abnormal growths.
These factors narrow the spinal canal, compressing nerves and causing stenosis symptoms.
What are the risk factors of spinal stenosis?
Age: Risk increases with aging.
Genetics: Family history matters.
Congenital: Narrow canal from birth.
Injuries: Past spine trauma or surgery.
Lifestyle: Heavy lifting, certain jobs.
Obesity: Excess weight strains spine.
Diseases: Arthritis, diabetes, etc.
Scoliosis: Abnormal spine curvature.
What are the red flag symptoms/signs of back pain?
Neurological Issues: Weakness, numbness, or tingling.
Bladder/Bowel Problems: Loss of control.
Severe Pain: Unbearable or unrelenting.
Fever: Along with back pain.
Unexplained Weight Loss: Rapid and unintended.
Cancer History: Especially if pain is new.
Night Pain: Worse at night.
Trauma: After injury or accident.
Age Over 50: New-onset pain.
Steroid Use: Especially long-term.
-
NeuroSurgStroke
Doctor Instruction:
Your patient is Charlie, a 63-year-old man presenting with problems with speech. Please take a history and carry out a relevant examination.
Patient History:
Charlie, 63y/o M, Engineer.
Your partner noticed a few hours ago that you were difficult to understand while speaking during dinner. Your speech has been slurred, according to your partner, and it happened very suddenly. Your partner was really worried about this and therefore called an ambulance.
You have noticed you cannot see things on your left which is “kinda weird” – you have never experienced this before in the past – you have to constantly rotate your neck to the side to see more. You also feel tired and not “really yourself”. You noticed you could not pick up your fork with your left hand or lift your left leg up when you tried to walk. These symptoms have not settled since then.
You are unsure whether you have swallowing difficulties, but you ate fine before slurred speech kicked in. No dizziness/ unsteadiness/ numbness/ headache/ confusion/ loss of consciousness/fever.
Ideas, Concerns, Expectations:
You think this might be another "ministroke". You had this last year which quickly resolved. You think you are likely to get better because of this. You have no concerns – you don't know why your partner was so concerned about this. You just want to go home and don't want to miss out on watching your favourite TV show.
Past Medical History:
Hypertension, atrial fibrillation, obesity, hypercholesteremia, previous “ministroke” x1 last year. Had a hernia operation in 2014.
Drug History:
Atorvastatin, aspirin, amlodipine, ramipril, apixaban.
NDKA
Family History:
Father had a heart attack when he was 50
Social History:
You live with your partner in a semi-detached house.
You work as an engineer.
You smoke 10 cigarettes a day since when you were a teenager (can't remember for how long exactly).
you drink a pint of beer every weekend.
Examination Findings:
Slurred speech
Left-sided weakness for arm and leg
Left homonymous hemianopia
No higher cerebral dysfunction (dysphasia, visuospatial disorder)
Differentials:
Stroke – likely ischaemic PACS ( Ischaemic stroke (87%) vs Haemorrhagic stroke (13%) )
Stroke – other forms
TIA
Investigations:
Observations + neuro observations
ECG / Echo – to rule out cardiac cause
Bloods: glucose (exclude hypoglycaemia), U&Es (neurological signs + exclude renal failure), FBC (r/o anaemia or infection), coagulation screen with INR
USS doppler carotids – rule out aortic stenosis
Non-contrast CT Scan (immediate) – to determine management: ischaemia vs haemorrhage
For further investigations: MRI Scan/CTA/MRA
Management:
Conservative:
Smoking cessation
Dietary changes
Lose weight
Exercise
Alcohol Control
Manage risk factors/co-morbidities: hypertension, hypercholesteremia, diabetes, AF, obesity, high cholesterol level…etc.
Rehabilitation (MDT: PT + OT + SALT + Nurses+ Dietician + social services + Optometry/Opthalmology + psychology + Orthotics)
Neuro observations + monitor with supportive care.
Maintain target oxygen saturation
Medical:
Referral to hyperacute/acute stroke unit.
Ischaemia:
Thrombolysis (<4.5 hours from onset) – alteplase if ischaemic and intracranial haemorrhage has been excluded (repeat CT scan needed post-thrombolysis to rule out haemorrhage complication).
Alternative: mechanical thrombectomy (6-24 hours of onset)
Antiplatelet therapy with PPI (e.g. STAT aspirin 300mg after CT and continued for 2 weeks – to be switched to clopidogrel 75mg lifelong for secondary prevention of stroke)
Statin e.g. atorvastatin 80mg life-long for secondary prevention
Haemorrhagic:
Withhold blood thinners
Urgent referral for neurosurgical assessment
Control blood pressure.
Consider reversal of anticoagulation.
Viva Questions:
What are the risk factors for stroke?
High blood pressure (hypertension)
Smoking
Diabetes
High cholesterol levels
Heart disease
Obesity and lack of physical activity
Poor diet
Excessive alcohol consumption
Age and gender (risk increases with age and is higher in men)
Family history and genetics
Previous stroke or transient ischemic attack (TIA)
Certain medical conditions (e.g., sickle cell disease)
Sleep apnea
Certain medications (e.g., hormone-based contraceptives)
What is the ROSIER scale?
The ROSIER (Recognition of Stroke in the Emergency Room) scale is a clinical tool used to aid in the early recognition and diagnosis of stroke, particularly within the emergency room setting. It's designed to help healthcare professionals quickly assess the possibility of a patient experiencing a stroke and facilitate prompt intervention. The scale evaluates specific signs and symptoms commonly associated with stroke.
The ROSIER scale typically considers various criteria, including facial weakness, arm weakness, speech disturbance, and age, to determine the likelihood of a patient having a stroke.
What are the indications for immediate CT Head?
Acute Head Trauma: Significant head injury.
Stroke or TIA: Focal neurological deficits or suspected stroke.
Subarachnoid Hemorrhage: Sudden severe headache.
Intracerebral Hemorrhage: Sudden severe neurological symptoms.
Mass Lesion or Tumor: New-onset or worsening neurological symptoms.
Infections or Abscesses: Suspected intracranial infections.
Hydrocephalus: Symptoms of increased intracranial pressure.
Vascular Abnormalities: Suspected aneurysms or AVMs.
Altered Mental Status: Sudden mental status changes.
Seizures: Prolonged or atypical seizures.
Severe Headaches: Sudden severe or atypical headaches.
Ophthalmologic Symptoms: Acute visual disturbances.
Post-Operative Patients: Recent neurosurgery with acute symptoms.
What are the key cerebellum defect signs?
Ataxia: Uncoordinated movements and balance issues.
Dysmetria: Difficulty judging distances accurately.
Intention Tremor: Shaking during purposeful movements.
Speech Disturbances: Slurred or abnormal speech rhythm.
Nystagmus: Involuntary rhythmic eye movements.
Vertigo or Dizziness: Sensation of spinning or unsteadiness.
Wide-Based Gait: Feet spaced apart for stability.
Incoordination of Movements: Difficulty with precise motions.
Tremor: Rhythmic shaking or quivering movements.
Reflex Abnormalities: Altered reflex responses (reduced or increased).
Tell me about the Bamford classification of ischaemic stroke.
The Bamford classification categorizes ischemic strokes into four types based on their clinical presentation:
Total Anterior Circulation Infarct (TACI): Severe deficits involving at least two areas (leg, arm, face, higher cortical functions).
Partial Anterior Circulation Infarct (PACI): Moderate deficits that don't meet TACI criteria.
Posterior Circulation Infarct (POCI): Involves brainstem and/or cerebellum, causing specific symptoms.
Lacunar Infarct (LACI): Small, deep infarcts causing motor or sensory deficits.
-
OrthopedicCauda Equina Syndrome
Doctor Instruction:
You are currently a senior surgical doctor on call. Your next patient is a 45-year-old gentleman, Adam, who presents back pain after being hit by a slow-moving car yesterday. Please take a history and perform an appropriate examination.
Patient History:
Adam, a 45-year-old gentleman, banker
You came in today following a small car collision towards your back while walking across the road last night. You brushed this off – thinking it was no big idea. However, you started noticing lower back pain with weakness in your lower limbs.
Back pain is located centrally in the lower back – can sometimes radiate down both legs. You describe the pain as sharp, rating it 10/10. You tried many things to ease the pain without success e.g. paracetamol and ibuprofen. Back pain can be triggered by simple back movement but not worsened by coughing or straining. You have numbness and tingling sensation running down both of your legs.
Also, while wiping yourself afterwards in the toilet, you couldn’t feel the sensation around your bottom as well as your genitals– it was very strange, and at that point, you knew you needed to go and seek medical attention. You developed incontinence for passing urine and faeces. You no longer have the urge to go the toilet, and they can come out involuntarily, which is very concerning for you—no other previous back injuries.
Idea, Concern, Expectation:
You have no idea what is going on, but you think it is related to yesterday's injury. You are very concerned and don’t want to be paralysed – you are still very young! You would like to find out what is going on. You are very scared if you need any surgery for this.
Past Medical History:
Hypertension, obesity
Drug History:
Ramipril, Atorvastatin
NKDA
Family History:
Ankylosing Spondylitis
Social History:
Smoke 10 cigarettes/day for over 20 years
Drink around 2-3 pints of beer every weekend
Work as a banker
Live with a wife and two kids in a semi-detached house
Examination Findings:
Both lower limbs power 4/5 with reduced sensations, tone, and reflexes.
Lower back spinal tenderness at L3/4 region.
PR Examination: Reduced anal tone and sensation.
No upper motor neurone signs
Differentials:
Caudal Equina Syndrome caused by trauma
Prolapsed lumbar disc
Conus medullaris syndrome
Mechanical back pain
Peripheral neuropathy
Spinal tumour
Investigations:
Basic observations
Routine bloods for baseline and pre-assessment e.g. FBC, U&Es, LFT, Bone Profile, CRP
Consider blood culture if suspected infection.
Emergency MRI to confirm and exclude cauda equina syndrome
Consider CT myelography/spine
Consider XR spine
Consider Urodynamic studies -to monitor bladder function
Management (Cauda Equina Syndrome):
Hospital Admission
VTE prophylaxis
Prevention of further damage e.g. Immobilise spine if CES is due to trauma
Neurosurgical input for consideration of lumbar decompression surgery – the earlier this is performed, the higher the chance of regaining functions.
Surgery may involve removing bone fragments, tumour, herniated disc, blood, debulking for SOL e.g. tumour abscess…etc.
Anti-inflammatories such as steroids, if due to inflammatory cause
For infectious causes, patients should be treated with antibiotics
Postoperative care includes physiotherapy, occupational therapy, and addressing lifestyle issues e.g. obesity.
Treatment for metastatic spinal cord compression includes analgesia, high-dose dexamethasone, surgery, radiotherapy, and chemotherapy. Investigations include biopsy, staging CT, PET scan…etc.
Viva Questions:
Explain the pathophysiology of cauda equina syndrome.
Cauda equina syndrome is caused by compression of nerve roots at the base of the spine. This pressure leads to severe back pain, leg pain, numbness, weakness, and bladder/bowel dysfunction.
Why is cauda equina syndrome a surgical emergency?
Cauda equina syndrome is a surgical emergency because the compression of nerve roots can cause permanent and severe neurological damage. Prompt surgery is essential to prevent irreversible loss of sensation, muscle function, and bladder/bowel control. The urgency is to minimize lasting deficits and improve patient outcomes.
Where does the spinal cord terminate (at what level)?
The spinal cord typically terminates around the level of the first or second lumbar vertebra (L1-L2) in most adults. Below this point, the spinal cord transitions into a bundle of nerve roots known as the cauda equina, which continues down the vertebral canal and provides innervation to the lower extremities and pelvic organs
What is conus medullaris?
The conus medullaris is the tapering, lower end of the spinal cord. It is located at the termination of the spinal cord, usually around the level of the first or second lumbar vertebra (L1-L2). Below the conus medullaris, the spinal cord transitions into the cauda equina, a bundle of nerve roots that extend further down the spinal canal. The conus medullaris is an important anatomical landmark and holds significance in medical imaging, surgical procedures, and discussions related to spinal cord and neurological health.
What are the causes of cauda equina syndrome?
Cauda equina syndrome is caused by conditions that compress or damage the nerve roots at the base of the spinal cord. Common causes include herniated discs, spinal tumors, spinal stenosis, trauma, infections, inflammatory conditions, and postoperative complications. Immediate medical attention is crucial to prevent permanent nerve damage.
Does cauda equina syndrome show lower or upper motor neurone signs or both?
Cauda equina syndrome leads to signs and symptoms characteristic of lower motor neuron involvement. These include bilateral reduction in sensation of the lower limbs, impaired bladder and bowel function, weakness in the lower limb muscles, intense back pain, and potential issues with sexual function.
-
OrthopedicAdhesive Capsulitis (Frozen Shoulder)
Doctor Instruction:
You are currently a senior surgical doctor on call. Your next patient is called Bob, a 41-year-old gentleman presenting with shoulder stiffness. Please take a history and perform an appropriate examination.
Patient History:
Bob, a 41-year-old gentleman, construction worker.
A few weeks ago, your left shoulder started becoming stiffer than usual, affecting movements in all directions; stretching exercises help with stiffness slightly, but stiffness is the same throughout the day. This is causing problems for you as you now need help with overhead activities and putting on your clothes. You feel like your left shoulder can no longer move as it used to with a limited range of motions.
Six months ago, you had a gradual worsening, constant left shoulder pain, which is often worse at night affecting your sleep- however, this is slowly getting better, so you are not too concerned, and you have a high pain tolerance. You describe the pain as a dull ache - rating it 2/10 currently. No radiation. No previous recent injury or known trigger. You tried many painkillers, such as paracetamol, with only minimal effects.
Idea, Concern, Expectation:
You have no idea what is going on. You work in construction, so this may be related. You had a few injuries towards your left shoulder in the past but nothing major. You are concerned as your work often involves very active use of your left shoulder, and you now have problems at work due to stiffness. You would like to see if you can have a sick note for this.
Past Medical History:
Type 2 diabetes, hypothyroidism
Previous left shoulder rotator cuff injury, which was treated conservatively three years ago.
No previous surgical history
Drug History:
Metformin, levothyroxine.
Allergic to fish - Rash.
Family History:
Mother has osteoarthritis affecting both hips.
Social History:
Work as a builder
Non-smoker
Drink around 3-5 units a week over a weekend.
Live with wife in a flat
Examination Findings:
Left shoulder stiffness on both active and passive movement in all directions with limited range of motions. However, external rotation is most affected. The whole shoulder joint is mildly tender to palpation.
Positive coracoid pain test - tenderness with direct pressure on the coracoid
Positive shoulder shrug test - inability to abduct arm to 90degree in the plan of body and to hold the position.
No tenderness at acromioclavicular joint. No painful arc on shoulder abduction.
Negative for other manoeuvres or shoulder tests.
Differentials:
Adhesive capsulitis (pain phase transitioning to stiff phase)
Supraspinatus tendinopathy
Acromioclavicular joint arthritis
Glenohumeral joint arthritis
Things to consider: septic arthritis, inflammatory arthritis, malignancy e.g. osteosarcoma, bony mets, fractures, shoulder dislocation, rotator cuff injury...etc.
Investigations:
Clinical diagnosis
Consider routine bloods if indicated to rule out other pathologies
Consider shoulder XR shoulder e.g. may show signs of arthritis
Consider ultrasound, CT, MRI (may show thickened joint capsule in adhesive capsulitis)
Management:
Conservative:
Continue using the left arm but don't exacerbate the pain
Encourage active/passive exercises and stretching
Analgesia e.g. paracetamol, NSAIDs
Physiotherapy
Psychosocial support
Consider transcutaneous electrical nerve stimulation (TENS) machine for pain management
Consider referral to pain clinic/orthopaedics if significant disability and poor pain control despite conservative/ medical management
Medical:
Intra-articular steroid injections
Consider short-term oral steroids
Surgical:
Hydrodilation (injecting fluid into joint to stretch capsule)
Manipulation under anaesthesia to improve range of motion
Arthroscopy, e.g. keyhole to remove adhesions and release shoulder
Arthroscopic capsulotomy
Viva Questions:
Explain the pathophysiology of adhesive capsulitis.
Adhesive capsulitis, or frozen shoulder, involves inflammation in the shoulder joint. This triggers collagen buildup and adhesion formation in the joint capsule, leading to stiffness and restricted movement. Over time, inflammation subsides, but adhesions persist, causing ongoing limited range of motion. Physical therapy and treatments aim to break down adhesions and improve shoulder function. In severe cases, medical interventions may be necessary.
What are the different phases of adhesive capsulitis?
Freezing Phase: Pain and stiffness increase as inflammation sets in.
Frozen Phase: Pain stabilizes, stiffness intensifies due to scar tissue and adhesions.
Thawing Phase: Pain and stiffness decrease, range of motion improves gradually.
How long can adhesive capsulitis generally last?
Adhesive capsulitis can last from a few months to a couple of years, with treatment playing a role in its duration. Early intervention and therapy can help shorten the recovery time.
What manoeuvre/ test can be used to test for supraspinatus tendinopathy?
The Empty Can Test (Jobe's Test) is used for supraspinatus tendinopathy. The person raises arms forward at 90 degrees, thumbs down. Downward pressure is applied, and pain or weakness suggests a potential issue with the supraspinatus tendon.
What are the complications of frozen shoulder?
Complications of frozen shoulder include prolonged stiffness, pain, loss of function, muscle imbalances, reduced quality of life, secondary issues in other body parts, chronic pain, limited work and activities, and emotional distress. Timely treatment and therapy can help prevent or minimize these complications.
What is the usual prognosis for frozen shoulder?
The prognosis for frozen shoulder varies, but with proper treatment and therapy, most individuals can expect gradual improvement over several months to years. Early intervention and consistent care can lead to full or nearly full recovery of range of motion and function. In some cases, residual stiffness or recurrence can occur, and underlying health conditions can influence outcomes.