administrators
Private
Posts
-
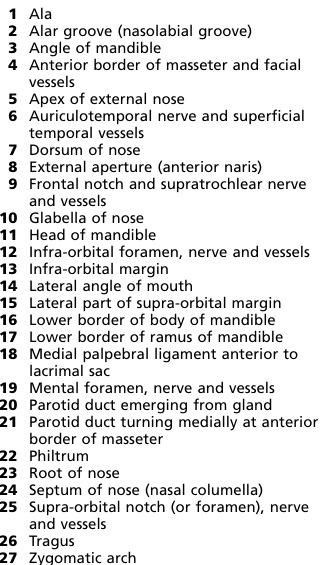
isb11 Face surface markings -
isb11 Face surface markings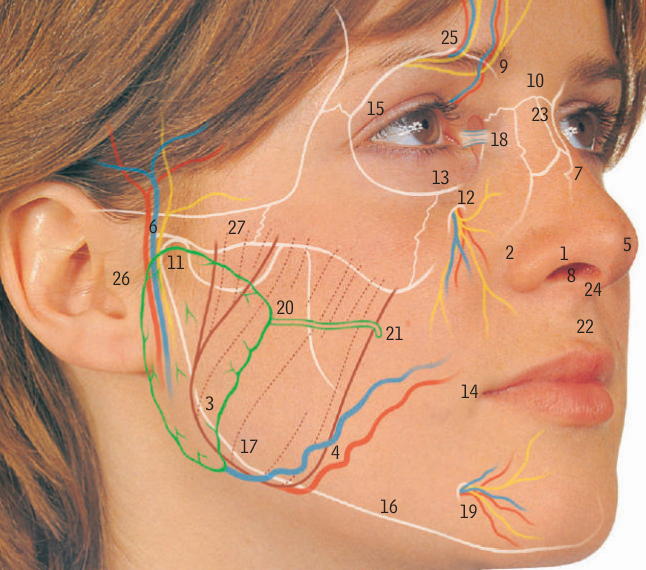
-
isb2 Neck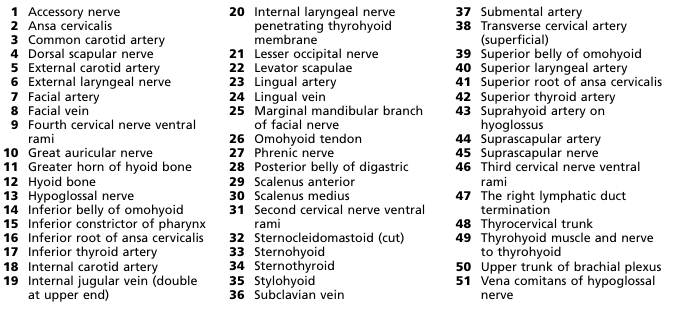
-
isb2 Neck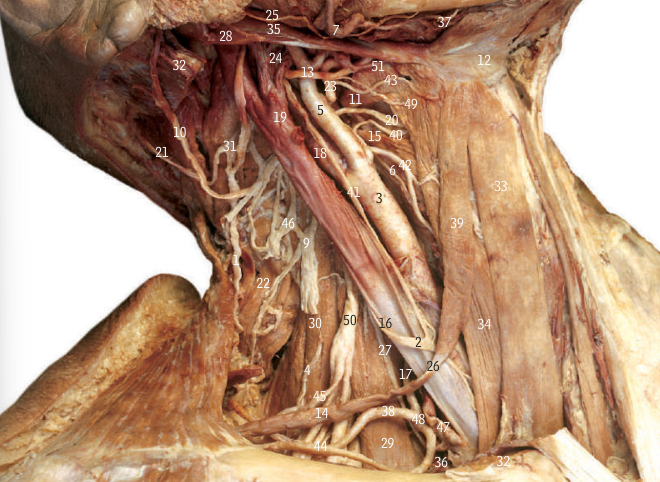
-
Post-Op reactive depressionPRESENTATION
John, a 56-year-old occupation, previously fit/smoker/social drinker who is on his 5th POD following ... [e.g. right hemicolectomy], has showed signs of anhedonia, depression and fatigue. He has also showed some signs of positive core biological symptoms.
Considering all of this, my provisional diagnosis is reactive (postoperative depression), I will also consider major
depressive disorder, bipolar disorder.What will be your management?
For mild conditionRegular exercise
Advice on sleep hygiene (regular sleep times, appropriate environment)
= Psychosocial therapy -CBT
Moderate to severeRegular exercise, advice on sleep hygiene
CBT
Medication -SSRIs
High-intensity psychosocial intervention (CBT or interpersonal therapy)
Immediate and considerable high risk to themselves or others: Admit to psychiatric ward (use Mental Health
Act if necessary) -
Post-Op reactive depression- Introduce yourself
Hello, good morning, I’m Dr. X, one of the surgical doctors today. How are you doing today?In this station, the patient is hospitalized and is now in postoperative period. So, you will not ask for name or age or Past medical or surgical history, Drug history, Family history, Ideas, concerns and expectations, other system review. |
- Obtain verbal consent
Would you mind if ask you some questions regarding your conditions?- Main history - [Divided into_3 segments that you have to assess; Core symptoms of depression, biological
symptoms of depression, past psychiatric history |
A. Core symptoms of depression (depression, anhedonia and fatigue)
* In the past days during your hospital stay * Have you felt down, depressed or hopeless? (Depression) * Found that you no longer enjoy, or find little pleasure in life? (Anhedonia) * Been feeling overly tired? (Fatigue)B. Biological symptoms of depression (mnemonic SMALL)
SleepHow has your sleep pattern been recently? Have you had any difficulties in getting to sleep? Do you find you wake up early, and find it difficult to get back to sleep?Mood
Are there any particular times of day that you notice your mood is worse? Does your mood vary throughout the day? Do you find that your mood gradually worsens throughout the day?Appetite
Have you noticed a change in your appetite? What is your diet like at the moment? What are you eating on a typical day?Libido (Seek permission again — I'm asking you some personal questions that include about your sexual life, and it would help me to reach a diagnosis and help you out. Whatever the information you give me, it will remain
confidential between us. Are you okay with this?)* Have you noticed any change in your libido? * Since you have been feeling this way, have you noticed a difference in your sex drive?C. Past psychiatric history - Previous episodes of depression or dysthymia
Have you ever felt like this before? Have you ever had any other periods of feeling particularly low? In the past, have you had any problems with your mental health? Have you had any counselling for any issues before? Have you ever been admitted to hospital because of your mental health? If so, obtain details -time, method of admission, result.POSITIVE FINDING
Positive core and biological symptoms of depression. -
Post-Op reactive depressionSTEM 1 - You are asked to take the history John, a middle-aged male on the 5th post-op day who has presented with low mood for 6 hours and loss of appetite. He is not willing to talk to anyone and seems to be lost, The nursing staff informs you that he has been sleeping poorly post-operatively.
-
Renin Angiotensin AldosteroneMedical song: RAAS
-
Difficult to say medical words@uninvitedguest@piefed.ca
Hi, yes AI tools used, with some human input.
What would you think is a better name for the channel?