Vagus nerve course in thorax & abdomen?
Thorax:
Left vagus nerve
SpoilerCrosses in front of the left subclavian artery. Enters the thorax between the left common carotid and subclavian arteries.
Descends on the left side of the aortic arch. Travels behind the phrenic nerve.
Courses behind the root of the left lung. Deviates medially and downwards to reach the esophagus and form the esophageal plexus with the right vagus nerve.
Right vagus nerve
SpoilerCrosses in front of the first part of the subclavian artery.
Travels behind the innominate vessels. Reaches the thorax on the right side of the trachea.
Inclines behind the hilum of the right lung. Courses medially towards the esophagus to form the esophageal plexus with the left vagus nerve.
Abdomen:
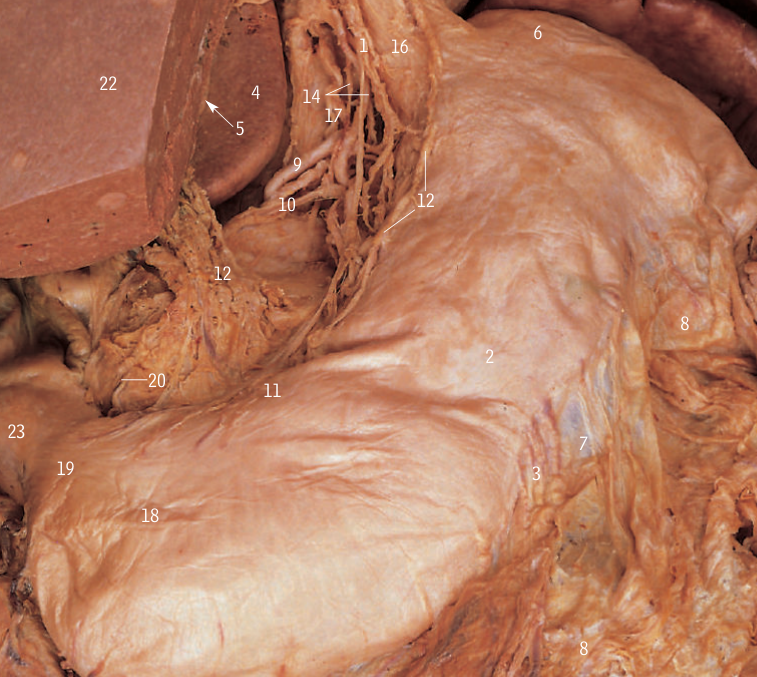
SpoilerThe oesophageal plexus, formed by the union of the right and left vagus nerves, The vagus nerve enters the abdomen through the oesophageal hiatus at the level of the tenth thoracic vertebra (T10).
It divides into the anterior and posterior vagal trunks, which innervate the stomach, small intestine, liver, gallbladder, pancreas, and spleen.
Nerves in oesophageal hiatus?
SpoilerAnt & post vagal trunks.
What do they supply?
SpoilerStomach, duodenum, jejunum, ileum, cecum, ascending colon, medial 2/3 of transverse colon, spleen, pancreas, gall bladder
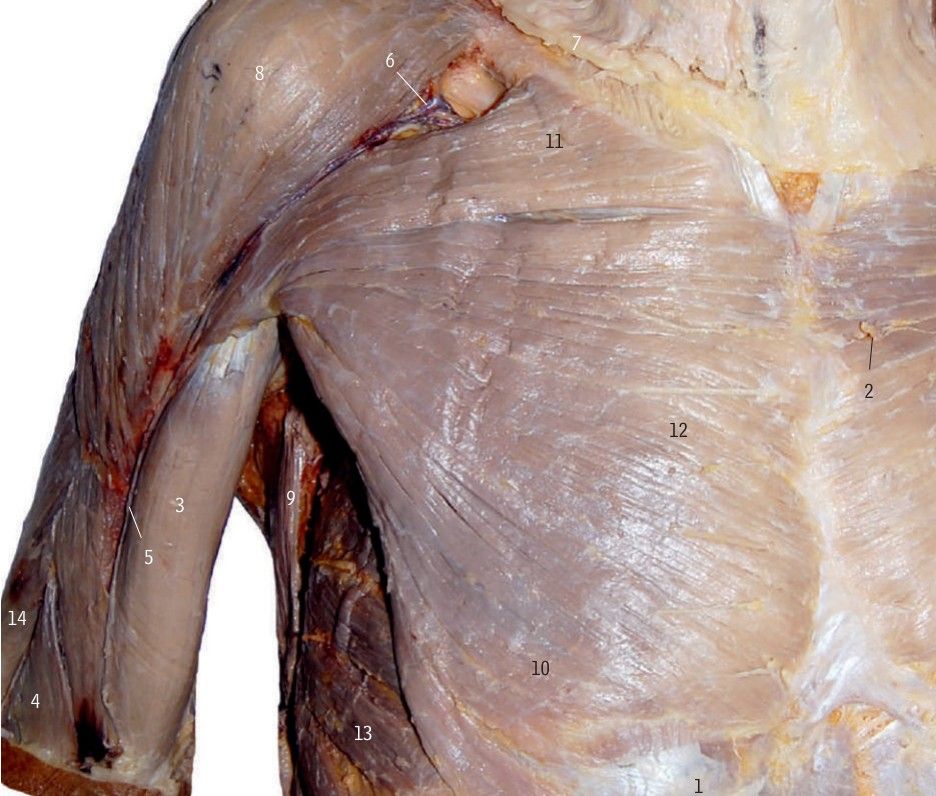
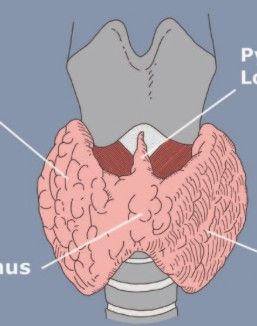
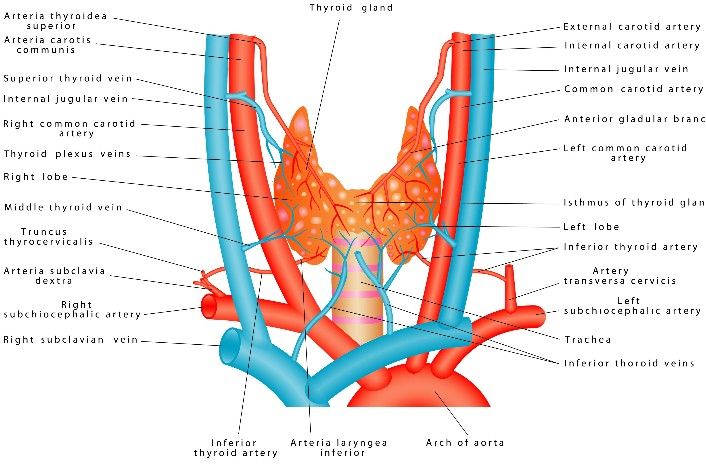
Muscle dissected to see thyroid?
SpoilerSternohyoid muscle