What is the most common part of the duct that is involved in a stone?
SpoilerMiddle 1/3
Why is this site most affected?
SpoilerDue to looping of lingual nerve around duct, and thick mucus secretion and have to pour secretion in floor of mouth against gravity
What are digastric triangle boundaries and their nerve supply?
SpoilerSuperior: Inferior border of the mandible
Anterior: Anterior belly of the di gastric muscle
Posterior: Posterior belly of the digastric muscle
Nerve supply
SpoilerThe anterior belly of the digastric muscle is innervated by the mylohyoid nerve, which is a branch of the mandibular nerve
The posterior belly of the digastric muscle is innervated by the digastric branch of the facial nerve.
Names & actions of extrinsic muscles of the tongue
SpoilerGenioglossus: protrusion of the tongue & depression of the tongue tip
Hyoglossus: retraction of the tongue & depression of the lateral margins of the tongue
Styloglossus: retraction of the tongue & elevation of the sides of the tongue
Palatoglossus: Elevation of the posterior part of the tongue
If you have injury of Hypoglossal, lingual or marginal mandibular what will the patient have?
Marginal mandibular
SpoilerDrippling of saliva from corner of affected side
Poor speech articulation (slurred speech)
Asymmetry on smiling or crying
Hypoglossal
SpoilerParalysis and atrophy in ipsilateral side
Deviation to ipsilateral side on protrusion
Poor speech articulation
Lingual
SpoilerLoss of general sensation from ant 2/3 of tongue and floor of mouth
Loss of taste sensation from tongue only
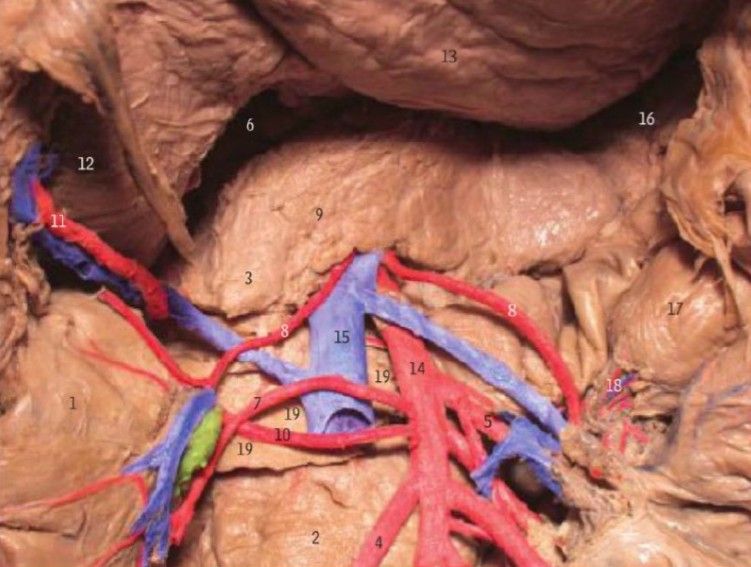
Boundaries of Posterior Triangle
SpoilerBoundary Description
Apex Sternocleidomastoid and the Trapezius muscles at the Occipital bone
Anterior Posterior border of the Sternocleidomastoid
Posterior Anterior border of the Trapezius
Base Middle third of the clavicle
[image: 1773944974415-596e7a43-c73e-42b3-bc28-fcbd5be83066-image.jpeg]
Origin & Insertion of Omohyoid
SpoilerOrigin - Insertion
Inferior belly
superior border of scapula near suprascapular notch - intermediate tendon
Superior belly
intermediate tendon - body of hyoid bone
Study Notes
Hypoglossal nerve
SpoilerBecause the genioglossus muscle on the healthy side "pushes" the tongue, it will deviate toward the side of the injury when the patient sticks it out.
Why lingual nerve injury causes loss of taste, even though it primarily carries general sensation?
SpoilerWhile the Lingual nerve is a branch of the Mandibular nerve and carries general sensation (touch, pain, temperature), it also acts as a "highway" for taste fibers.The Chorda Tympani Connection. The reason a lingual nerve injury (specifically if it occurs after the two nerves join) causes loss of taste is due to the Chorda Tympani, a branch of the Facial nerve (CN VII). The Join: High up in the infratemporal fossa, the Chorda Tympani "hitches a ride" with the Lingual nerve. The Shared Path: From that point forward, they travel together as one physical cord.
Omohyoid, remember that its two bellies are held together by an intermediate tendon. This tendon is actually tethered to the clavicle by a deep layer of fascia. This is why when the muscle contracts, it doesn't just pull the hyoid down; it also helps maintain the patency of the internal jugular vein!