Gen Surg
-
Inflammatory Bowel Disease
Doctor Instruction:
You are currently a senior surgical doctor on call. Your next patient is Anna, a 20-year-old university student complaining of abdominal pain. Please take a history and perform a relevant examination.
Patient History:
You noticed a dull generalised abdominal pain that started in the past week. It is gradually getting worse. It does not radiate. The pain is not worsened/improved with eating or defecation. Pain score 6-7/10.
You also noticed diarrhoea starting 3 days ago, passing 4-5 loose and “mucusy” stools daily, but no blood. Stools are not particularly foul-smelling. You have lost around 1-5 kg over this period. Similar episodes have come and gone repeatedly for the past year. You are well between episodes, but feel very low and run-down during episodes. You also have a sore mouth, but you've had frequent mouth ulcers since childhood. You feel feverish but haven’t taken a temperature yet.
You cannot recall eating anything troublesome before this, but generally, you eat a low-fibre and highly processed food diet. No recent antibiotics, hospital admissions or foreign travel. No nausea/vomiting, dysphagia, jaundice, weight loss, or fever. No joint pains or skin rashes.
Ideas, Concerns, Expectations:
You think you might have IBS, which your flatmate also has. You're worried you might have caught this from her and about the impact this pain has been having on your university studies, and you want to know how long the pain will take to resolve (ask the doctor directly).
Past Medical History:
Fit and well.
Drug History:
None.
NKDA.
Family History:
You recall your mother had a similar problem but can’t remember exactly what caused this. You have a family history of diabetes (not sure which type).
Social History:
You are a university student studying interior design.
You live with your flatmate.
You smoke 5-10 cigarettes daily and drink 2-3 units per week.
Examination Findings:
Oral aphthous ulcers
Generalised abdominal tenderness with no guarding.
Tender, red, raised nodules on the shins consistent with erythema nodosum
PR examination may elicit pain and reveal perianal lesions e.g. fistula, skin tags, abscesses…etc.
Differentials:
Inflammatory bowel disease (Crohn’s disease most likely)
Gastroenteritis
Irritable bowel syndrome
Coeliac disease
To rule out causes of acute abdomen e.g. appendicitis, bowel obstruction, pancreatitis, perforation…etc
Investigations:
Bedside:
Baseline observations (pyrexia + tachycardia)
Stool sample = culture, faecal calprotectin, C.diff toxin
Bloods:
FBC + iron studies/b12/folate (anaemia due to blood loss or iron/B12 deficiency)
U&E, Mg, Ca (dehydration > kidney injury, nutritional deficiencies)
LFT (baseline before starting medications, IBD associated with hepatobiliary disease e.g. gallstones in Crohn’s, PSC in Ulcerative colitis)
CRP/ESR (raised in active IBD)
TPMT (checked before starting thiopurines)
Anti-TTG with serum IgA levels (coeliac disease)
Amylase (rule out pancreatitis as a cause for abdominal pain)
B-hCG
Imaging:
XR abdomen to assess severity, rule out causes of abdomen pain
CT/MRI abdomen (to look for complications e.g. fistulas, abscesses and strictures)
Special Test:
OGD / Colonoscopy with biopsy (diagnostic)
Management (IBD):
Conservative:
MDT approach e.g. IBD specialist nurse, gastroenterologist…etc.
Stool chart
Assess nutritional status +/- dietician input
Smoking cessation
Antispasmodic agents e.g. dicycloverine, hyoscyamine
Antidiarrheal agents e.g. loperamide
Medical (referral to gastroenterology):
Crohn's Disease:
Inducing remission:
Steroids (oral prednisolone/IV hydrocortisone, 2nd line: azathioprine, methotrexate, infliximab, adalimumab
Maintain remission:
Azathioprine or mercaptopurine, 2nd line: methotrexate, infliximab, adalimumab
Ulcerative Colitis:
Inducing remission:
Mild to moderate disease: aminosalicylate e.g. mesalazine PO/PR, 2nd line: corticosteroids e.g. prednisolone
Severe disease: IV hydrocortisone, 2nd line IV cyclosporin
Maintaining remission:
Aminosalicylate e.g. mesalazine, azathioprine, mercaptopurine
Surgical:
Crohn's disease:
When the disease only affects the distal ileum, this can be resected surgically to prevent a flare-up of the disease – however, Crohn's disease often involves the entire GI tract. Strictures and fistulas secondary to Crohn’s disease can be managed by surgery.
Ulcerative colitis:
Panproctocolectomy (removal of colon and rectum) forming either an ileostomy or an ileoanal anastomosis
Viva Questions:
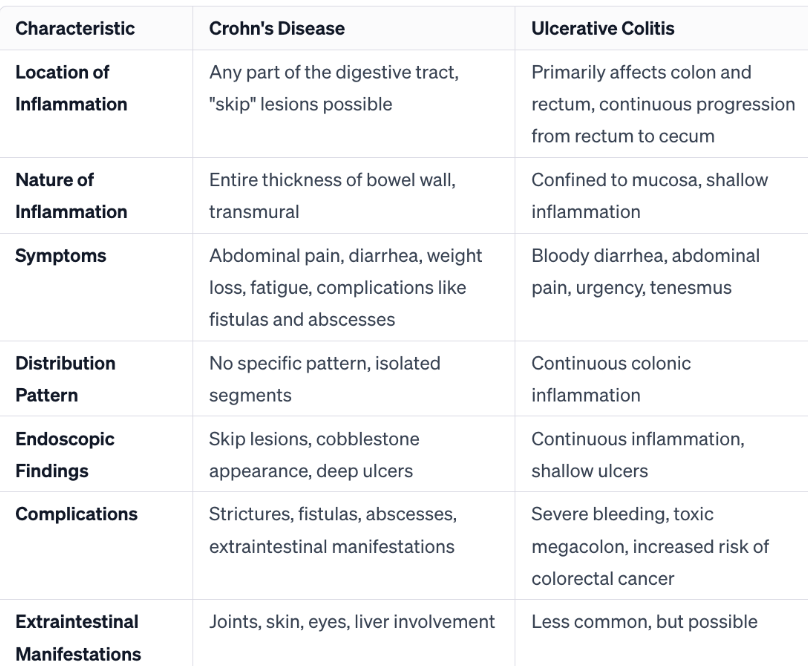
How do you differentiate Crohn’s from Ulcerative colitis?
What are the extra-intestinal manifestations of IBD?
Joint Problems (Arthritis):
Inflammatory arthritis, often peripheral, and less commonly axial involvement.
Skin Conditions:
Erythema nodosum, pyoderma gangrenosum, and psoriasis.
Eye Inflammation:
Uveitis and episcleritis, causing redness, pain, and blurred vision.
Liver Involvement:
Primary sclerosing cholangitis (PSC), especially associated with ulcerative colitis.
Kidney Stones:
Increased risk due to dehydration and calcium absorption changes.
Osteoporosis:
Resulting from chronic inflammation and corticosteroid use.
Blood Disorders:
Anemia due to chronic inflammation or nutrient deficiencies.
Peripheral Neuropathy:
Nerve inflammation leading to tingling, numbness, or weakness.
Deep Vein Thrombosis (DVT) and Pulmonary Embolism:
Increased risk of blood clots.
Oral Health Issues:
Aphthous stomatitis, contributing to mouth ulcers.
-
Appendicitis
Doctor Instruction:
You are currently a senior surgical doctor on call. Your next patient is Ben – a 23-year-old male presenting with abdominal pain. Please take a history and perform a relevant examination.
Patient History:
Ben - 23-year-old gentleman - Master Student.
You experienced sudden tummy pain 12 hours ago. This is getting worse, so you have decided to go to the A&E to check it out. The pain is centralised at the lower right quadrant of your tummy. You describe this as excruciating sharp pain – rate it as 8/10. Moving around and touching the site of pain makes it more painful. You have tried to take some paracetamol, but it doesn't seem to work that much.
If asked specifically, the pain you remember started only around your belly button and moved to the lower right quadrant 3-5 hours ago.
You have lost your appetite but try to eat/drink whenever you can. You are experiencing both nausea and vomiting. No blood in the vomit - just normal food you have eaten. You feel quite warm + feverish, and you notice your face has gotten redder than usual. You haven't been to the toilet to empty your bowel for >24 hours. No blood in the stool. Your waterworks are normal.
Ideas, Concerns, Expectations:
Yesterday, you ate some raw sashimi with your mates at a new Japanese restaurant in town. You are not sure if you have caught an infection because of this. You know you have a weak stomach compared to your peers, and that's why you are the only one feeling unwell. Your other mates are well and healthy. You are very concerned as this pain is no longer tolerable. You can't even move and do anything. You want some morphine to ease the pain.
Past Medical History:
Crohn's disease, asthma
Drug History:
Steroids for Crohn’s disease, salbutamol inhaler as required.
NKDA
Family History:
Mother has Crohn’s disease.
Social History:
Currently, a master's student studying architecture.
You are currently living in a flat shared with your mates.
You are not managing at home at the moment.
You do not smoke.
You drink around two cans of beer every weekend with the lads.
Examination Findings:
Inspection: unwell, in pain, sweating, flushed face, doesn’t want to move
Lower right quadrant tenderness – McBurney’s sign
Rebound tenderness at right iliac fossa +/- Guarding
Reduced bowel sounds
Psoas sign positive (right)
Rovsing’s sign positive
Differentials:
Appendicitis (classic history and examination findings)
Appendix mass
Gastroenteritis (fever + recent uncooked meal)
Crohn’s disease flare (PMH + FH)
Investigations:
Bedside:
Observations
Stool MCS– rule out gastroenteritis
Bloods:
FBC – mild leucocytosis in appendicitis
U&E – dehydration from vomiting
LFT – baseline + rule out other causes of abdominal pain
CRP – inflammation
Blood culture - infection
Group and Save - to prepare for theatre
Imaging:
Contrast CT Abdomen – appendicitis, rule out other pathology i.e. bowel obstruction/perforation
US – appendicitis / ovarian cysts if female + first line for young patients
Other investigations to consider:
Urinalysis - to rule out UTI as cause for pain
Pregnancy test if female (Ectopic pregnancy)
Abdominal MRI
Management:
Immediate senior surgical review
Nil by mouth
Consider Drip and suck
Analgesia i.e. IV paracetamol 15mg/kg / IV morphine 5-10mg
Antibiotics if not fit for surgery or evidence of infection e.g. IV amoxicillin 500mg + IV metronidazole 500mg – initiate sepsis if appropriate.
Surgery: appendicectomy + prophylactic antibiotics under local protocols
Emergency appendicectomy if suspected perforation
Viva Questions:
Explain the pathophysiology of appendicitis.
Appendicitis is the inflammation of the appendix, a small, finger-like pouch located at the beginning of the large intestine. The pathophysiology of appendicitis involves obstruction of the appendix, leading to bacterial overgrowth, inflammation, and eventually infection. The obstruction can occur due to factors such as fecaliths (hardened stool), lymphoid hyperplasia, or tumors.
When the appendix becomes obstructed, mucus and bacteria accumulate within the appendix, causing increased pressure. This pressure leads to impaired blood flow and oxygen supply to the appendix, resulting in tissue damage and inflammation. As inflammation progresses, the appendix swells, and the immune response intensifies.
What age ranges do people tend to get appendicitis?
Appendicitis can occur at any age, but it is most common in people between the ages of 10 and 30. The condition is relatively rare in children younger than 2 years old and adults older than 30. However, appendicitis can still occur outside these age ranges, and individuals of any age should be aware of the symptoms.
What is Rovsing's sign?
Rovsing's sign is a clinical test for appendicitis. It involves applying pressure to the lower left abdomen; if this causes pain in the lower right quadrant, it is considered a positive sign.
What are the signs of peritonitis?
Peritonitis is inflammation of the peritoneum, the thin tissue lining the inner wall of the abdomen and covering most abdominal organs. Signs and symptoms of peritonitis can include:
Abdominal pain: Typically, the pain is severe and may be diffuse or localized to the area of infection.
Tenderness: The abdomen is often tender to the touch.
Abdominal distension: Swelling or bloating of the abdomen may occur.
Fever and chills: Elevated body temperature is common, along with chills.
Nausea and vomiting: These symptoms may be present, often accompanied by a lack of appetite.
Fluid in the abdomen (ascites): In some cases, there may be an accumulation of fluid in the abdominal cavity.
Increased heart rate (tachycardia) and rapid breathing (tachypnea): These are signs of the body's response to infection and inflammation.
Decreased urine output: Reduced urine production may occur due to decreased blood flow to the kidneys.
How would you treat appendix mass?
The treatment of an appendix mass, also known as an appendiceal mass or phlegmon, is typically managed conservatively in the initial phase. This approach involves addressing inflammation and infection without immediate surgery. The treatment plan may include:
Antibiotics: Administering intravenous antibiotics to combat the infection and reduce inflammation.
NPO (Nil per os): Keeping the patient NPO means restricting oral intake to allow the digestive system to rest. Intravenous fluids may be provided for hydration.
Pain management: Using pain medications to alleviate discomfort.
Close monitoring: Regular monitoring of vital signs and clinical status to ensure improvement and to watch for any signs of worsening.
Imaging studies: Performing imaging studies such as CT scans to assess the extent of inflammation and to guide treatment decisions.
Surgery: General surgeon to determine the appropriate timing for potential appendectomy (surgical removal of the appendix) after the acute phase has subsided.
In some cases, the inflammation may resolve with conservative treatment, and surgery may not be necessary. However, if there is a recurrent episode or persistent symptoms, surgical intervention (appendectomy) may be recommended to prevent future complications.
What are the complications of appendicectomy/surgery in general?
Appendectomy complications may include infection, bleeding, adverse reactions to anesthesia, organ damage, blood clots, respiratory issues, ileus, hernia, and abscess formation. Laparoscopic surgery may carry additional risks. While these complications are uncommon, the decision for surgery considers the overall risk-benefit balance.
-
Hernia
Doctor Instruction:
You are currently a senior surgical doctor on call. You are asked to see Wan, a 35-year-old accountant, complaining of a lump in his groin. Please take a history and perform a relevant examination.
Patient History:
It's all a bit embarrassing, really, but you've got a groin lump. You noticed the lump last week, and it's been there ever since. It's like you've got a tennis ball under your skin. It's making things like wearing pants very awkward and sometimes a bit uncomfortable. You haven't noticed any change in size with coughing, straining or standing for prolonged periods. It was uncomfortable to touch.
You've come in today because you've been getting waves of 5/10 abdominal pain today at the site. Paracetamol didn't seem to make much of a difference. You've been feeling sick on and off, and actually vomited once this morning - just normal food content. You last opened your bowels the night before yesterday and passed urine as normal without straining. There was no blood in your stool. You have had no difficulty swallowing, indigestion, fever or weight loss.
Ideas, Concerns, Expectations:
You are not sure what this is. You can concerned the lump is cancer. You wish to get it checked out.
Past Medical History:
Appendicectomy 10 years ago. Asthma.
Drug History:
Ventolin inhaler PRN. Steroid inhaler.
NKDA.
Family History:
None.
Social History:
You are currently working as an accountant. It's good work, and you're able to work from home, so you have plenty of time to go to the gym for your weightlifting.
You don't smoke or drink.
You live with your wife and two young girls at home, where you are normally independent.
Examination Findings:
Left groin mass superior and medial to the pubic tubercle 2x2cm soft
Tender on palpation at the hernia site.
Non-reducible. Non-pulsatile
Positive cough impulse
No guarding or signs of peritonitis.
Differentials:
Direct inguinal hernia
To rule out bowel obstruction/ perforation
Incisional hernia if the site of hernia is at the site of incision for appendicectomy
Vascular e.g. saphena varix, femoral artery aneurysm. (would be pulsatile).
Subcutaneous e.g. lipoma, sebaceous cyst.
Lymphoma
Investigations:
Clinical diagnosis. If uncertain, can use ultrasound as first line.
Other abdominal imaging - AXR (bowel dilatation/ free air), CT Abdo (look for obstruction/bowel perforation)
Management:
In asymptomatic and reducible cases, conservative management is an option with general surgery follow-up.
He will require surgery e.g. open/laparoscopic mesh repair if there's a high risk of complications when hernia is incarcerated/ causing bowel obstruction/ strangulated/ irreducible. For this, he will need admission and preparation for surgery e.g. NBM, IV fluids, catheterise, fluid balance, VTE prophylaxis, analgesia...etc.
Viva Questions:
What are the risk factors for the development of an inguinal hernia?
The main risk factors for inguinal hernia development include:
Age: Risk increases with age.
Gender: Men are more susceptible.
Family History: Genetic predisposition.
Premature Birth/Low Birth Weight: Higher risk in such cases.
Chronic Cough or Straining: Increases intra-abdominal pressure.
Obesity: Excess weight strains abdominal muscles.
Heavy Lifting: Especially if done improperly.
Pregnancy: Especially with multiple pregnancies.
Ascites: Fluid accumulation in the abdomen.
Previous Abdominal Surgery: Weakens abdominal muscles.
How do you differentiate between a femoral and inguinal hernia? Between a direct and indirect inguinal hernia?
Location:
Inguinal Hernia: This type of hernia occurs in the inguinal canal, which is a passage in the lower abdominal wall. Inguinal hernias are further divided into two types: direct and indirect:
Direct Inguinal Hernia: This hernia occurs when abdominal contents push through a weakened area in the lower abdominal wall, often in the Hesselbach's triangle.
Indirect Inguinal Hernia: This hernia occurs when abdominal contents protrude through the deep inguinal ring and into the inguinal canal. It may follow the pathway of the descent of the testes during fetal development.
Femoral Hernia: This type of hernia occurs lower down in the groin area, just below the inguinal ligament. It protrudes through the femoral canal, which is a passageway through which blood vessels and lymphatics pass.
Anatomy:
Inguinal Hernia: Inguinal hernias are more common in both men and women. They are located in the inguinal region, which is near the groin and may cause a bulge in the scrotum in men or the labia in women.
Femoral Hernia: Femoral hernias are more common in women, especially those who have been pregnant. They occur just below the inguinal ligament and may cause a bulge in the upper thigh.
Talk me through your examination for inguinal hernia.
Patient Positioning: Stand, expose groin with chaperone.
General Inspection: Check for asymmetry, swelling, or skin changes.
Scrotal Examination: Inspect for masses, tenderness.
Palpate along inguinal canal.
Cough test for dynamic assessment.
Differentiate Hernia Types: Direct vs. Indirect.
Auscultation: Listen for bowel sounds over the hernia.
Documentation: Record size, location, tenderness, and dynamic changes.
Repeat examination with the patient lying down.
What are the causes of bowel obstruction?

-
Acute Cholecystitis
Doctor Instruction:
You are currently a senior surgical doctor on call. Your next patient is Katie, a 45-year-old lady complaining of abdominal pain. Please take a history and perform a relevant examination.
Patient History:
You have some dreadful pain below your right ribs; it started gradually before you went to bed last night. But it's suddenly much worse today. It is a constant deep but sharp 7/10 pain in your right upper quadrant. You've been feeling the pain shooting up to your back on the right. Nothing seems to make it worse, and nothing's improving it either!
This isn't the first time you've had tummy pain. For the past few months, you've been getting episodes of sharp pain in that area, which usually lasts a few hours and then goes away, usually starting after lunch. You've been taking ibuprofen for the pain. But the pain this time is different, and you don't feel like yourself at all!
You vomited once about four hours ago and have generally been sick. You've had no change to your bowels. You last opened your bowels this morning. The stool was not pale and wasn't difficult to flush. You have no jaundice. You have chronic reflux, and no recent changes have happened. No difficulty swallowing. You haven't had any cough or chest pain.
Gynae-wise, you haven't had any issues, your last period was two months ago, but they have been a bit irregular recently – you wonder why! No problems with waterworks thankfully!
You have been feeling hot and flushy this morning. You haven't noticed any recent changes in your weight. You cannot recall eating anything troublesome before this.
Ideas, Concerns, Expectations:
You were warned by your GP that you were at risk of getting ulcers because of your reflux, so you're worried this is what's going on. The pain is quite severe, and you just want to get something stronger than ibuprofen.
Past Medical History:
GORD
NAFLD
Drug History:
Omeprazole
Allergic to penicillin (swollen mouth)
Family History:
None.
Social History:
You are an office worker, but you've been working from home this past year and have gained quite a bit of weight.
You also broke up with your partner last year, so you now live alone in a flat.
Your diet isn't the greatest, often buy fast foods and the occasional Indian takeaway.
You stopped smoking 3 years ago but restarted smoking about 10 cigarettes a day last year.
You occasionally drink alcohol, but nothing over 5-6 units per week.
Examination Findings:
Sweaty and hot to touch
Tachycardic (104bpm)
No jaundice
Abdomen tender to light palpation
Murphy's positive (only mention if tested or whilst palpating for hepatomegaly)
Abdominal aorta palpable and pulsatile, not expansile
Differentials:
Cholecystitis (RUQ pain on a background of biliary colic associated with fever in the absence of jaundice. Worry about associated sepsis)
Other biliary pathology e.g. biliary colic, choledocholithiasis, cholangitis
Peptic ulcer disease (history of reflux and taking ibuprofen)
Ectopic pregnancy
Hepatitis
Pancreatitis
Investigations:
Bedside:
Vital signs (shock, sepsis)
Pregnancy test
Bloods:
FBC (bleeding ulcer, infection)
U&E (dehydration, AKI)
LFT (obstructive picture, bilirubin levels)
CRP/ESR (infection)
Amylase (pancreatitis)
Imaging:
Abdominal USS (look for gallstones, gallbladder wall thickening and surrounding fluid)
MRCP
Erect CXR (perforated PUD)
AXR (Rigler's sign may indicate perforated PUD)
Endoscopy
Management:
Conservative:
NBM + surgical preparation
Stop ibuprofen and advise against it in cases of reflux - consider a PPI trial of increasing dose of omeprazole.
Medical:
Analgesia
Antibiotics (according to local guidelines for pen allergy)
Surgical:
Urgent laparoscopic cholecystectomy
Viva Questions:
What is the Charcot's triad?
Charcot's triad is a set of three classic symptoms that are traditionally associated with acute cholangitis, a condition characterized by inflammation and infection of the bile ducts. The triad includes:
Fever: Patients with acute cholangitis often experience an elevated body temperature, which is a common sign of infection.
Jaundice: Jaundice refers to the yellowing of the skin and eyes. In acute cholangitis, the inflammation and obstruction of the bile ducts can lead to impaired bile flow, resulting in the accumulation of bilirubin in the bloodstream and causing jaundice.
Right Upper Quadrant Abdominal Pain: Pain or discomfort in the right upper quadrant of the abdomen is another component of Charcot's triad. This pain is often associated with inflammation and distension of the bile ducts.
What are the risk factors for developing cholecystitis?
Risk factors for cholecystitis include gallstones, age (over 40), female gender, obesity, rapid weight loss, pregnancy, diabetes, genetic predisposition, certain medical conditions (such as Crohn's disease), and specific ethnic backgrounds (Native American or Mexican American).
How does cholecystitis cause shoulder tip pain?
Cholecystitis can cause shoulder tip pain due to referred pain involving the phrenic nerve. Inflammation of the gallbladder irritates the diaphragm, and the shared nerve pathways, particularly the phrenic nerve (C3-C5), can lead to the brain interpreting pain signals from the diaphragm as originating from the shoulder area.
What is Murphy's sign, and what does it indicate?
Murphy's sign is a clinical test for gallbladder inflammation (cholecystitis). It involves placing fingers below the right costal margin and asking the patient to take a deep breath. If pain and cessation of inhalation occur due to gallbladder tenderness, the test is positive, suggesting possible cholecystitis, often caused by gallstones. Additional diagnostic tests are usually needed for confirmation.
Name some complications of cholecystitis.
Gangrenous Cholecystitis: Severe inflammation can lead to tissue death in the gallbladder wall.
Perforation: Inflammation may cause the gallbladder to rupture, leading to bile leakage into the abdominal cavity.
Abscess Formation: Pus collection within or around the gallbladder.
Bile Duct Obstruction: Inflammation or gallstones can obstruct the common bile duct, affecting the flow of bile.
Pancreatitis: Inflammation of the pancreas can occur due to the spread of inflammation from the gallbladder.
Empyema: Accumulation of infected pus within the gallbladder.
Gallstone Ileus: Large gallstones can migrate into the intestine, causing a bowel obstruction.
Sepsis: Severe infection that can spread throughout the body.
-
Bowel Obstruction
Doctor Instruction:
You are currently a senior surgical doctor on call. Your next patient is a 56-year-old gentleman (Adam) coming in due to vomiting. Please take a history and perform a relevant examination.
Patient History:
Your name is Adam – You are currently 56-year-old – retired, and used to work as an accountant.
Since yesterday you have been vomiting, and it is only worsening – you also noticed you were starting to vomit green stuff today, which looked horrible and shocked you! Vomit doesn't contain any blood/faecal matter. You have been struggling to keep food down. You have a poor appetite. You feel weak and tired. You haven't had a good sleep since yesterday.
You also started to develop sudden, intermittent excruciating tummy pain throughout your tummy, which is widespread. No radiation. Pain score 9/10. You tried to take paracetamol and Oramorph, but it didn't help. Any movement only makes the pain worse, so you try to stay still as much as possible. You also feel your tummy has gotten a little bigger than usual. You do not feel well at all. You feel feverish with some chills.
You have not been passing bowel content/wind in the past week. No diarrhoea or bloody stool recently. No weight loss. No night sweats. No recent infection / surgery/ admission. No recent weight loss.
Ideas, Concerns, Expectations:
You are not sure what is going on. You don't think you have eaten anything abnormal lately. Maybe you have some constipation. You are concerned that the pain is now getting worse today. You hope to find out what is going on and receive some medications to help control your pain!
Past Medical History:
Hypothyroidism, type 2 diabetes, appendectomy, cholecystectomy, previous inguinal hernia operation, paroxysmal atrial fibrillation
Drug History:
Levothyroxine NKDA, metformin, apixaban
NKDA
Family History:
Bowel cancel >60 years old, diverticular disease
Social History:
You smoke 10 cigarettes/ day for the last 20 years.
You drink about 1-2 pints of beer every week.
You use oramorph recreationally, but you haven't been taking this last week until the pain started.
You live in a house with your partner currently.
Examination Findings:
Patient looks uncomfortable. Generalised abdominal tenderness – worst at the umbilical region. Voluntary guarding suggesting peritonitis. Bowel sound is absent. Abdominal distension with hyper-resonant on percussion. No palpable mass/lump. Previous surgical scars are present.
Signs of dehydration might include prolonged capillary refill time, tachycardia, reduced skin turgor, and dry mouth.
Differentials:
Bowel obstruction secondary to e.g. adhesions (due to extensive history of abdominal surgeries), strangulated hernia, malignancy, volvulus…etc.
Need to rule out bowel perforation
Bowel ischemia
Diverticular disease
Gastroenteritis
Acute pancreatitis
Constipation e.g. secondary to opioid use/ dehydration / hypothyroidism
Investigations:
Bedside:
ABCDE assessment
Observation (tachycardia, hypotension / pyrexia may indicate perforation/ infarction)
ECG (tachycardia/ rule out arrhythmias)
ABG (metabolic alkalosis/electrolyte imbalance due to vomiting + raised lactate if bowel ischaemia)
Fluid charts for input/out monitoring/ consider catheterisation (may show signs of dehydration e.g. oliguria)
BM /ketones (DKA/HHS)
Urinalysis (rule out UTI cause of abdominal pain / may show high ketones for DKA)
Admit all patients with bowel obstruction/ perforation
Urinalysis
Serum hCG in women of childbearing age.
Bloods:
FBC(high WCC/neutrophilia, low haematorcrit or hb indicates blood loss), CRP, LFTs, U&Es (electrolyts imbalance from vomiting/ reduced kidney function from dehydration/ pseudoobstruction), Bone Profile, Amylase, Lactate, Cross-match / cross match (for surgery / plan for blood transfusion), serum/urine osmolality (HHS), blood culture (for suspected infection)
Imaging:
Supine and erect XR Abdomen (rule out gas in peritoneum/ bowel dilatation / may show fluid level)
Barium swallow (can also be therapeutic)
Erect CXR (rule out referred pain from pneumonia/ gas under diaphragm)
Consider water-soluble contrast enema XR for diagnosis
CT scan (rule out obstruction + perforation or other causes of abdominal pathology/plan for surgery)
Consider MRI / US for diagnosing bowel obstruction or other causes.
Special Test:
Consider endoscopy e.g. flexible sigmoidoscopy/colonoscopy (can be diagnostic/therapeutic e.g. stenting) Care should be taken due to the risk of perforation / exacerbating complications. Should be in the absence of sepsis/ ischaemia/ perforation/ peritonitis/ closed loop obstruction/ abscesses/ distal rectal lesions/ persistent coagulopathy, dilated caecum more than 9cm.
Management:
Conservative:
Urgent referral to General Surgery for suspected bowel obstruction
Nil by mouth + bowel rest
IV fluids resuscitation
Consider NG tube for persistent vomiting / prevent aspiration
Electrolyte replacement if appropriate
Consider dietician input
Ice to suck to moisten mouth and lips / reduce the sense of thirst
Analgesia e.g. morphine sulphate
VTE assessment and prophylaxis
Consider conservative approach e.g. watchful waiting in incomplete obstruction, previous surgery suggesting ?adhesion, advanced malignancy, pseudo-obstruction, sigmoid volvulus?
Avoid stimulant laxatives if the patient has colic/ stop all laxatives in complete obstruction
Consider antiemetics – Care should be taken for prokinetic metoclopramide
Medical:
Consider (prophylactic) antibiotics in those with suspected perforation / bowel ischaemia / for surgery.
Consider neostigmine to aid recovery of intestinal pseudo-obstruction alongside with correction of fluid and electrolyte imbalance
Surgery
Consider endoscopy for bowel decompression, dilatation of strictures via stenting for patients in palliative care or awaiting elective surgery
Consider sigmoidoscopy + passage of flatus tube in sigmoid volvulus without perforation or decompression via colonoscopy in caecum volvulus / pseudo-obstruction.
Early laparotomy/ laparoscopic surgery e.g. exploratory surgery/ adhesiolysis/ hernia repair/ resection if persisting obstruction, ischaemic, perforation / peritonitis/ irreducible hernia / palpable mass + failure to improve. Ischaemic bowel may require resection. A stoma may be created following an operation
Post-op care
Prior to discharge, advise on diet, emotional changes, weight management, adapting physical activity, expectation for recovery, smoking/alcohol use, when and where to seek help if appropriate.
Palliative such as in those with advanced malignancy and unfit for surgery:
Analgesia
Antiemetics
Antispasmodics
Antisecretory
Corticosteroids e.g. dexamethasone (may reverse partial obstruction)
Colonic stenting
Viva Questions:
What are the different types of bowel obstruction and their likely causes?
Small Bowel Obstruction:
Adhesive obstruction (scar tissue after surgery)
Hernia (protrusion through weakened abdominal wall)
Volvulus (twisting of the small intestine)
Intussusception (telescoping of intestine)
Strictures (narrowing due to inflammation or scarring)
Large Bowel Obstruction:
Colorectal cancer
Diverticulitis (inflammation or infection of diverticula)
Strictures (narrowing due to scarring)
Volvulus (twisting of the colon)
What is paralytic ileus?
Paralytic ileus is a condition where normal muscle contractions in the gastrointestinal tract are temporarily disrupted, leading to a slowdown or cessation of movement of contents. It can result from surgery, inflammation, infection, medications, or other medical conditions. Symptoms include abdominal bloating, nausea, vomiting, and constipation. Treatment involves addressing the underlying cause, supportive care, and, in severe cases, surgery.
What are the complications of bowel obstruction?
Ischemia (Lack of Blood Supply): Obstruction can compromise blood flow to the affected segment of the bowel, leading to ischemia. Prolonged ischemia can result in tissue damage and necrosis (death of tissue).
Bowel Perforation: Increased pressure within the obstructed bowel can cause the bowel wall to rupture, leading to bowel perforation. This can result in peritonitis, a severe inflammation of the abdominal cavity.
Sepsis: Bowel perforation can lead to the release of bacteria and digestive contents into the abdominal cavity, causing infection. Severe infection can progress to sepsis, a life-threatening condition.
Fluid and Electrolyte Imbalances: Vomiting, dehydration, and the loss of fluids into the obstructed bowel can lead to imbalances in electrolytes (such as sodium and potassium) and dehydration.
Malnutrition: Prolonged obstruction can lead to malabsorption of nutrients, causing malnutrition.
Distension and Rupture of the Bowel: Obstruction can cause significant distension of the bowel, leading to increased pressure. In severe cases, the distended bowel may rupture.
Renal Failure: In some cases, bowel obstruction can lead to reduced blood flow to the kidneys, potentially causing kidney dysfunction or failure.
Respiratory Complications: Severe abdominal distension can affect diaphragmatic movement, leading to respiratory difficulties.
Shock: In cases of severe complications, such as bowel perforation and sepsis, the patient may go into shock, which is a life-threatening condition characterized by inadequate blood flow to vital organs.
Give some examples of how a "closed loop" obstruction may occur?
Closed-loop bowel obstruction can occur in various ways:
Adhesion Formation:
Scar tissue from surgery causes the bowel to close at two points.
Volvulus:
Twisting of the bowel at two points leads to a closed loop.
Intussusception:
Telescoping of the bowel results in closure at both ends.
Hernia:
Trapped bowel within a hernia forms a closed loop.
Internal Herniation:
Bowel herniates internally, creating a closed loop.
What are the upper limits of normal diameter of the bowel e.g. small bowel, colon, and caecum?
Normal bowel diameter can vary among individuals and may be influenced by factors such as age, body size, and imaging technique. However, there are general reference ranges for the normal diameter of the small bowel, colon, and cecum which can be measured in imaging like XRays:
Small Bowel:
Normal diameter: Less than 3 cm
Large Bowel:
Normal diameter: Up to 6 cm
Cecum:
Normal diameter: Up to 9 cm
What XR findings would you expect to see in large bowel obstruction vs small bowel obstruction?
Large Bowel Obstruction (LBO):
Dilated Colon: Visible dilation of the large bowel with haustral markings.
Transition Point: Distinct transition point, often in the sigmoid colon or rectum.
Small Bowel Obstruction (SBO):
Dilated Small Bowel Loops: Multiple, uniformly dilated small bowel loops.
Valvulae Conniventes: Visible circular folds crossing the entire width of the small bowel.
"Umbilical" or "Triangle" Sign: Converging loops creating a triangle or "umbilical" shape.
How do you get third-spacing in bowel obstruction, and what is the complication of this?
In bowel obstruction, third-spacing occurs due to increased pressure within the obstructed bowel, causing fluid to move from blood vessels into surrounding tissues. Complications include dehydration, hypovolemic shock, electrolyte imbalances, and organ dysfunction.
What are the symptoms/signs of dehydration/hypovolaemia?
Thirst: Increased thirst is a natural response to fluid loss.
Dark Yellow Urine: Concentrated urine with a dark yellow color indicates reduced fluid intake.
Dry Mouth and Dry Skin: Insufficient fluid levels may lead to dryness of the mouth and skin.
Fatigue: Dehydration can cause fatigue and a feeling of weakness.
Dizziness or Lightheadedness: Reduced blood volume can affect blood pressure and lead to dizziness.
Rapid Heartbeat: The heart may beat faster to compensate for decreased blood volume.
Sunken Eyes: Dehydration may cause the eyes to appear sunken.
Infrequent Urination: Reduced fluid intake can result in decreased urine output.
Headache: Dehydration may contribute to headaches.
Confusion or Irritability: Severe dehydration can affect cognitive function and mood.
What are the different types of shock?
Shock is a life-threatening medical emergency characterized by inadequate blood flow to the body's tissues and organs. There are several types of shock, each with distinct causes and features:
Hypovolemic Shock:
Cause: Severe loss of blood or other fluids (e.g., from trauma, bleeding, dehydration).
Features: Rapid heart rate, low blood pressure, cold and clammy skin, confusion.
Cardiogenic Shock:
Cause: Heart-related problems, such as a heart attack, severe heart failure.
Features: Weak pulse, rapid breathing, cold and clammy skin, confusion.
Distributive (Vasodilatory) Shock:
Subtypes:
Septic Shock: Caused by severe infection leading to systemic inflammation.
Neurogenic Shock: Resulting from a disruption of the autonomic nervous system (e.g., spinal cord injury).
Anaphylactic Shock: Triggered by a severe allergic reaction.
Features: Vasodilation, low blood pressure, rapid heart rate, warm and flushed skin (except in neurogenic shock), respiratory distress.
Obstructive Shock:
Cause: Obstruction of blood flow due to a physical barrier (e.g., pulmonary embolism, cardiac tamponade).
Features: Signs vary based on the specific cause but may include difficulty breathing, chest pain, rapid heart rate.
-
Diverticulitis
Doctor Instruction:
You are currently a senior surgical doctor on call. Your next patient is a 51-year-old gentleman called Isaac, presenting with bloody stool. Please take a history and perform an appropriate examination.
Patient History:
Your name is Isaac – a 51-year-old – estate agent.
In the past three days, you have been having maroon-red diarrhoea with clots (not bright red or dark black, smelly stools). This is not settling or getting worse. You don't think you have eaten anything abnormally lately, but you generally eat a low-fibre diet. You did have some constipation a few days before having diarrhoea. You haven't noticed any lumps or bumps around your tummy. You have lost your appetite. Feeling sick and have been vomiting slightly (just food contact / no blood or bile). You also noticed aching pain on your tummy's lower left side. It comes on intermittently. Worsen by eating and improved slightly by emptying stool and passing gas. You feel your tummy is a little more bloated than usual. You also noticed you had been feeling warm with a bit of shivering last night. You do feel tired lately, but you are not sure whether this is from your stressful work or lack of sleep. You are not sure if you have lost any weight recently. Waterworks normal.
Ideas, Concerns, Expectations:
You have no idea what this might be. You hope it is not cancer – you have much more to live for! You are concerned because the stool is red; you might be bleeding somewhere in your bowels. You really want to know what is happening- your wife is concerned about this.
Past Medical History:
Ankylosing spondylitis, atrial fibrillation, diverticular disease, obesity, hypercholesterolaemia
Drug History:
Ibuprofen, apixaban, lansoprazole
Allergic to shellfish (rash)
Family History:
Ulcerative Colitis
Social History:
Ex-smoker – used to smoke 10 cigarettes a day for 10 years.
Drink a bottle of wine every other week.
Work as an estate agent.
Live with wife.
Examination Findings:
Lower left quadrant pain tenderness
No guarding or signs of peritonitis
No rebound tenderness
No hernia/ lump
No signs of testicular torsion
Bowel sound present
Murphy's sign negative
Rovsing's sign negative
PR exam – may show tenderness or mass suggesting pelvic abscess.
Differentials:
Diverticulitis +/- complications
IBD
Ischaemic colitis
Gastroenteritis
To rule out GI cancer
Other causes of abdominal pain to rule e.g. peptic ulcers (use of NSAIDs + apixaban)
Investigations:
Bedside:
Observations (pyrexia/ tachycardia)
ECG (tachycardia/rule out arrhythmias) +/- echo (cause of embolism/ valvular pathology)
Urine dip (rule out UTI as a cause of abdominal pain)
Bloods:
CRP/WCC (raised in diverticulitis)
Hb (blood loss- anaemia)
Lactate (raised in ischaemic colitis)
U&Es (baseline + urea raised in dehydration/GI bleeding)
CRP
Group and Save
Coagulation Screen (bleeding + ischaemia?)
Blood Culture if suspected infection/sepsis
LFT/Amylase (rule out abdominal pain causes)
Imaging:
XR Abdomen ( to look for dilated bowel loops, thumbprinting in ischaemic colitis…etc.)
Erect CXR (to rule out air under the diaphragm)
Urgent CT scan with contrast (aim with 24 hours) for suspected complicated diverticulitis + high CRP (alternative non-contrast CT, MRI, US)
Consider CT angiography for suspected bowel ischaemia (gold standard)
Special Test:
Colonoscopy (to confirm diagnosis/ rule out other possible diagnoses)
Flexible sigmoidoscopy (to rule rectosigmoid lesion)
If no bleeding source can be identified with sigmoidoscopy, consider a non-invasive approach e.g. (nuclear scintigraphy) or an invasive approach e.g. angiography/ colonoscopy to localise/treat the bleeding source.
Consider cystoscopy/ cystography, contrast radiographs or methylthionium chloride (methylene blue) studies for colovesciular fistula tracts.
Management:
Consider admission when:
Pain is not managed with simple paracetamol
Poor hydration with oral fluids
Oral antibiotics cannot be tolerated
Bleeding requiring transfusion
Frailty + significant comorbidities
Symptoms persist for over 48 hours despite conservative management at home
Features of complications
Conservative (especially in uncomplicated, asymptomatic diverticular disease – consider management at home +/- antibiotics if symptomatic + safety netting):
Rest
Bulk-forming / stimulant laxatives should be avoided
Nil by mouth or clear fluids only until symptoms improve
IV fluids/ hydration
Analgesia e.g. paracetamol – avoid NSAID / opioids if possible
Consider antispasmodic may for cramping
Consider NG/antiemetics if vomiting
Medical:
Consider Oral co-amoxiclav 625mg TDS (at least 5 days) – in uncomplicated diverticulitis but systemically unwell / immunosuppressed/ significant comorbidities (alternative: cefalexin + metronidazole)
Consider IV antibiotics in severe acute diverticulitis e.g. severe pain / complications (IV co-amoxiclav or IV cefuroxime + metronidazole) + stepping down regime following review in 48 hours / CT scan results)
Consider blood transfusion due to significant blood loss + stop blood thinning medication + consider vitamin K / tranexamic acids
Surgery:
General Surgery Input/ referral
Surgery may be required for complications e.g. perforation, purulent/faecal peritonitis, uncontrolled sepsis, peri-diverticular abscess, fistula, ileus, obstructions, haemorrhage…etc.
In free perforation with generalised peritonitis - it may involve urgent surgical laparoscopic lavage and resection surgery. Primary anastomosis +/- diverting stoma or Hartmann's procedure are standards for routine or emergency surgery.
Management of further complications:
Abscess might involve antibiotics, bowel rest, percutaneous drainage, and standard surgery.
Fistula – resection with fistula closure + repair
Obstruction- might involve resection, endoscopic balloon dilation, stenting
Haemorrhage – fluid/blood resuscitation, vasopressin, angiographic embolisation, surgery e.g. resection
Prevention:
High fibre diet e.g. fruits and vegetables, whole grain, good fluid intake + bulk-forming laxative, exercise, smoking cessation, weight loss
Viva Questions:
Explain the pathophysiology of diverticulitis?
Diverticulitis starts with the formation of pouches (diverticula) in the colon due to increased pressure and weakened colon walls. When fecal matter gets trapped in these pouches, it can lead to bacterial growth and inflammation. The immune system responds, causing further inflammation and potential complications like abscesses, perforation, and bowel obstruction. High pressure, low-fiber diet, and aging are key factors in this process.
What are the risk factors for diverticular diseases?
Aging (especially over 40)
Low-fiber diet
Lack of physical activity
Obesity
Smoking
Genetics (family history)
Previous history of diverticular disease
Connective tissue disorders
What are the complications of diverticulitis?
Abscess formation
Perforation (rupture)
Peritonitis (inflammation of the abdominal lining)
Fistula formation (abnormal connections)
Bowel obstruction
Stricture formation (narrowing of the colon)
Hemorrhage (severe bleeding)
Septicemia (bloodstream infection)
Psoas abscess (infection in the lower back muscle)
At what sites does diverticulum most occur in the GI tract?
Diverticula primarily occur in the sigmoid colon, followed by other parts of the colon, and rarely in other areas of the digestive tract.
-
Acute Pancreatitis
Doctor Instruction:
You are currently a senior surgical doctor on call. Your next patient is Guy – a 45-year-old gentleman presenting with abdominal pain. Please take a history and perform a relevant examination.
Patient History:
Your name is Guy – a 45-year-old gentleman who works in a pub.
You noticed in the past two days that you developed a sudden abdominal pain at the top of your tummy and the belly button region. It comes on intermittently, and it is worsening. You described the pain as dull. The pain also radiates towards the back (when this happens, you feel like you are being stabbed with a knife in the back) and is associated with vomiting (no blood/bile – just food content). The pain is 6/10. The pain is worsened by eating food in general. You have tried to use paracetamol to ease the pain, but it hasn't helped that much.
You have had a bad appetite since yesterday and haven't been eating or drinking. You feel sick when you eat – but haven't vomited yet. You are quite constipated lately (no blood/offensive smell in stool /diarrhoea otherwise in previous stools) – haven't been opening your bowel for around 3 days. The stool has not been paler lately or difficult to flush. No urinary problems.
You also have been a little more breathless, but you do not know why. No cough. No fever. No recent trauma. No recent surgery/ procedure. No recent infection. No itchy skin.
Ideas, Concerns, Expectations:
You think this is related to the gallstones. You had similar symptoms in the past. You are concerned if you need any surgery for this as last time, the doctor said they are considering gallbladder removal. You don't want any surgeries; your grandmother died during an operation. You would like to have something to ease the pain.
Past Medical History:
Known to have gallstones and fatty liver, polymyalgia rheumatica (recently diagnosed), hyperlipidaemia, heart failure
Drug History:
Started on steroids 2 days ago, omeprazole, furosemide, statin NKDA
Family History:
Rheumatoid arthritis, gallstones
Social History:
You drink around 2-3 cans of lager per day
Don’t smoke
Live by yourself
Work in a pub
Examination Findings:
Corneal arcus
Tachycardia
Warm peripherals
Appears to be Jaundice/icterus
Epigastric/ umbilical region tenderness with rigidity but no guarding (no signs of peritonitis)
Bowel sound reduced
No signs of ascites
Cullen's sign / Grey Turner's sign
Murphy's sign is negative
Mild pitting oedema bilaterally
Calves soft and non-tender
On chest auscultation – it may show signs of pleural effusion: localised reduced air entry and dullness to percussion/ coarse crackles at bases
Signs of dehydration may include dry mouth, reduced skin turgor, and prolonged capillary refill time
Differentials:
Acute pancreatitis secondary to alcohol/ gallstone/ steroid/ hyperlipidaemia
Cholangitis/ Cholecystitis
Rule out other causes of acute abdomen e.g. peptic ulcer
Decompensated heart failure
To rule out ARDS
To rule out AAA
Investigations:
Bedside:
Observations (low grade pyrexia / tachycardia/ hypoxia/ low sat)
ECG (tachycardia)
ABG e.g. PaO2, lactate, glucose (Glasgow score)
Bloods:
Pancreatitis Glasgow score includes in bloods: WCC (neutrophil) in FBC, LDH/ AST in LFTs, albumin + Calcium in bone profile, glucose, Urea in U&Es
Additionally: CRP (inflammation) + amylase/lipase (raised in pancreatitis – >x3 normal level for amylase, bilirubin in LFTs (may be raised) + other routine bloods to assess for baseline
Blood culture if signs of infection
Emerging test: Urinary trypsinogen-2 (elevated in pancreatitis), Serum IL-6/8 (if raised – may indicate severe risk of pancreatitis)
Imaging:
Abdominal XR (faecal loading / rule out obstruction / perforation)
CXR (acute respiratory distress syndrome / pleural effusions / basal atelectasis)
Ultrasound Abdomen/ endoscopic US (to assess for gallstone/dilated bile duct/ fluid collection/ pancreatic inflammation, peripancreatic stranding, calcification/ biliary sludge)
CT Abdomen +/- contrast – can be diagnostic / assess for complications of pancreatitis e.g. abscess/ fluid collections/pseudocyst/ necrosis + rule out lesions e.g. malignancy) + rule out other causes of acute abdomen
Consider MRCP in gallstone present/ dilatation of biliary tract for further assessment
Special Test:
Fine needle aspiration and culture/biopsy (infected pancreatic necrosis/ unknown lesion)
Management (Acute Pancreatitis):
Conservation:
Patient Education e.g. condition
Sociopsychology support
IV Fluids
Nil by mouth initially, and once symptoms are resolved/ improving blood tests – food can be introduced (consider a low-fat diet for patients with gallstones)
NG tube if severe vomiting
Antiemetics
Analgesia
Careful monitoring
Nutritional support / dietician input e.g. NG feed / TPN + electrolyte/vitamin replacement as appropriate(potential risk of refeeding syndrome)
Laxative if appropriate
Electrolyte replacement if appropriate
Oxygen when required (ARDS)
Medical:
Consider antibiotics if evidence of infection e.g. abscess / infected necrotic areas
Consideration for admission for high dependency unit (HDU) / Intensive care unit (ICU) for moderate/severe cases).
Surgical:
Consider ERCP+/- stenting/ cholecystectomy in gallstone pancreatitis
Treatment of complications e.g. endoscopic/ percutaneous drainage of collections + culture/sensitivity e.g. peritoneal fluid/ pseudocysts/ abscesses
To treat obstruction of biliary system / pancreatic duct e.g. pancreaticojejunostomy instead of ERCP
Removal of inflamed tissues + debridement of necrotic tissues/ pancreatoduodenectomy for pancreatic cancer/ other pancreatic resection procedures.
Newer management: pancreatectomy followed by islet cell transplantation
Long-term management:
Reduce / quit / prevent : alcohol/smoking / other risk factors e.g. via support group / lifestyle advice e.g. dietary
Consideration of replacement pancreatic enzymes (Creon) – for malabsorption
Consideration of subcutaneous insulin regimes if required for diabetes
Viva Questions:
Explain the pathophysiology of acute pancreatitis.
Acute pancreatitis begins with enzymes prematurely activating within the pancreas, causing tissue damage. This triggers inflammation, attracting immune cells and causing local effects like necrosis and pseudocysts. The inflammatory response can also affect other organs, potentially leading to multiple organ failure. Prompt diagnosis and treatment are essential to manage the condition and prevent severe complications.
What are the complications of pancreatitis?
Complications of pancreatitis can be serious and life-threatening. They include:
Necrotizing Pancreatitis: Severe inflammation leads to tissue death (necrosis) in the pancreas.
Pancreatic Abscess: Accumulation of infected fluid or pus within or near the pancreas.
Pseudocysts: Fluid-filled sacs containing pancreatic enzymes, blood, and tissue debris.
Organ Failure: Severe cases can cause failure of multiple organs, such as kidneys, lungs, or heart.
Sepsis: Widespread infection that can lead to a life-threatening systemic response.
Acute Respiratory Distress Syndrome (ARDS): Severe lung dysfunction due to inflammation.
Acute Kidney Injury: Sudden kidney dysfunction due to reduced blood flow or inflammation.
Disseminated Intravascular Coagulation (DIC): Abnormal blood clotting throughout the body.
Diabetes Mellitus: Damage to the pancreas can lead to long-term insulin production issues.
Chronic Pancreatitis: Continuous inflammation can lead to irreversible changes and chronic pain.
How do we assess the severity of pancreatitis?
Clinical: Evaluate symptoms and physical signs.
Lab Tests: Check amylase, lipase, CBC, LFTs, and renal function.
Imaging: Use CT, MRI, or ultrasound to visualize the pancreas.
Scoring Systems: Use APACHE-II, Ranson's Criteria, or Glasgow-Imrie Criteria.
Complications: Identify organ failure, necrosis, abscesses, or pseudocysts.
Monitor Progression: Watch for changes and treatment response to adjust care.
What are the potential causes of pancreatitis?
I: Idiopathic
G: Gallstone, Genetic - Cystic Fibrosis
E: Ethanol (alcohol)
T: Trauma
S: Scorpion sting or Spider bite
M: Mumps
A: Autoimmune conditions (like lupus)
S: Steroids
H: Hyperlipidemia or Hypercalcemia
E: ERCP (Endoscopic Retrograde Cholangiopancreatography)
 Drugs e.g. tetracycline, furosemide, azathioprine, thiazide.
Drugs e.g. tetracycline, furosemide, azathioprine, thiazide.Why is lipase more sensitive + specific than amylase for pancreatitis?
Lipase is preferred for diagnosing pancreatitis because it's more specific to pancreatic issues, has a longer detection window, and is more sensitive than amylase. It provides clearer results and is endorsed by clinical guidelines.
-
Haemorrhoids
Doctor Instruction:
You are currently a senior surgical doctor on call. Your next patient is a 45-year-old male called Alex, presenting with constipation. Please take a history and perform an appropriate examination.
Patient History:
45-year-old male, Alex, a bodybuilder.
In the past few weeks, you have been getting worsening constipation. You are not sure why. You usually eat healthily and avoid junk food. Yesterday, you noticed bright red blood on the toilet tissue paper while trying to wipe yourself, and you saw your stool was coated with fresh blood! You were very shocked because of this. You are not sure if this is yet another flare of your IBD - but you have no tummy pain, and you feel well. Your IBD is usually well controlled with azathioprine. Straining in the toilet can sometimes make your anus slightly sore – you feel like there’s something in your anus, but you are not sure if there's anything. You don’t want to look at your anus or feel around it with your finger – yuck! This grosses you out.
You do have a sensation that your back passage is always full, especially when you strain yourself, and this is starting to affect your ability to work out at the gym. You can sometimes soil yourself by chance – which is embarrassing!
Not sexually active currently. No weight loss. No night sweats. No abdomen pain. No nausea or vomiting. No fever. No SOB. No tiredness. Good energy level.
Ideas, Concerns, Expectations:
You have no idea what this might be; it might be another flare of your IBD. You are, however, worried that you might have cancer because your dad developed bowel cancer and died. You do not want to die so soon! You are still looking for the "one" to marry and happily live with!
Past Medical History:
Ulcerative colitis
Drug History:
Azathioprine.
Allergic to penicillin (anaphylactic reaction)
Family History:
Bowel cancer (father)
Social History:
You work in the gym and often travel to different countries to enter bodybuilding competitions – you have won so many trophies since you were a teenager - you are quite proud of your achievements. You live alone in a flat. You do not smoke or drink. You are generally independent and manage well at home.
Examination Findings:
The abdomen is soft and non-tender. Bowel sound present.
Digital Rectal Examination: non-tender wart-shaped swelling can be felt at the 3 o’clock position proximal to the anal verge – if ask the patient to strain, the swelling becomes visible at the anal verge- appearing bluish, bulging vessels covered with mucosa. No other internal/ external / prolapsed masses can be seen or felt. The prostate gland is normal. Normal anal tone. No PR bleeding or melena.
Differentials:
Haemorrhoid (non-thrombosed)
To rule out Colorectal Cancer
Inflammatory Bowel Disease
Anal Fissures
Diverticulosis
Investigations:
Observations (assess haemodynamic stability and rule out fever)
Proctoscopy to visualise swelling at the rectum
Consider FIT testing if rectal bleeding is not confirmed
Consider Faecal calprotectin – (higher level, more severe IBD)
Consider FBC + iron studies for anaemia (if prolonged PR bleeding + signs of anaemia/infection), CRP (raised in active IBD), baseline bloods: U&Es, LFT, Bone profile, coagulation screen.
Consider Colonoscopy / flexible sigmoidoscopy to exclude other serious pathology and confirm the diagnosis with biopsy i.e. IBD and cancer.
Consider anorectal physiological studies or anorectal US if associated with soiling/incontinence.
Management:
2ww referral if suspecting Lower GI Cancer
Simple analgesia e.g. paracetamol, ice packs if required
Topical treatment to reduce swelling/ pain of haemorrhoids: Anusol (astringent), Anusol HC (hydrocortisone), Hermoloids Cream (lidocaine), Proctosedyl Ointment (cinchocaine + hydrocortisone) - care should be taken how long the course should be
To treat constipation: increasing fibre in diet e.g. raw fruits, vegetables, fibre supplements, hydration, laxative when required – bulk-forming laxative such as ispaghula husk. Alternatives include lactulose or sodium docusate, avoiding straining while opening bowels, avoid too much caffeine or alcohol.
Non-surgical treatments of haemorrhoids: rubber band ligation (cut off blood supply by fitting a tight rubber band at the base of haemorrhoid), injection sclerotherapy (injection of phenol oil causing sclerosis and atrophy), infra-red coagulation (to damage blood supply of haemorrhoids), bipolar diathermy (electrical current to remove haemorrhoids)
Surgical treatment of haemorrhoids: haemorrhoidal artery ligation (cutting off blood supply), haemorrhoidectomy, stapled haemorrhoidopexy
Consider admission to those presenting with thrombosed haemorrhoids for excision under local anaesthetic/ incision and drainage of the clot
Viva Questions:
What are haemorrhoids?
Hemorrhoids, also known as piles, are swollen and inflamed veins in the lower rectum and anus. They can be internal (inside the rectum) or external (under the skin around the anus). Common causes include increased pressure on the veins due to straining during bowel movements, chronic constipation or diarrhea, pregnancy, obesity, and prolonged sitting or standing. Symptoms may include pain, itching, bleeding during bowel movements, and discomfort. Treatment often involves dietary changes, improved hygiene, topical creams, and in severe cases, procedures to remove or shrink the hemorrhoids.
What are thrombosed haemorrhoids?
Thrombosed hemorrhoids are swollen and painful veins in the anal area that have a blood clot. They cause severe pain, swelling, and a hard lump near the anus.
Where would you commonly find haemorrhoids in the rectum?
Hemorrhoids can occur throughout the rectum, but they are most commonly found at positions like "3 o'clock" and "9 o'clock" inside the anus (internal) or outside the anus (external).
What is the classification/grading of haemorrhoids?
Hemorrhoids are often classified or graded based on their severity and the extent to which they protrude from the anal canal. The most commonly used classification system is the one developed by Goligher, which categorizes hemorrhoids into four grades:
Grade I (First-degree hemorrhoids):
Hemorrhoids that bleed but do not prolapse (protrude) or cause any significant protrusion.Grade II (Second-degree hemorrhoids):
Hemorrhoids that prolapse during a bowel movement and retract spontaneously (go back inside) afterward.Grade III (Third-degree hemorrhoids):
Hemorrhoids that prolapse during a bowel movement and require manual repositioning (pushed back inside) afterward.Grade IV (Fourth-degree hemorrhoids):
Hemorrhoids that are always prolapsed and cannot be manually repositioned.What are the risk factors for haemorrhoids?
Straining during bowel movements: Putting excessive pressure on the rectal area.
Chronic constipation or diarrhea: Disrupting normal bowel movements can contribute.
Sedentary lifestyle: Lack of physical activity can lead to poor circulation and increased pressure on veins in the rectal area.
Obesity: Excess weight can contribute to increased pressure on the rectal veins.
Pregnancy and childbirth: The pressure on the abdomen during pregnancy and the strain of childbirth can increase the risk.
Aging: The risk increases with age due to weakened rectal tissue and veins.
Genetics: Family history of hemorrhoids may play a role.
Low-fiber diet: Insufficient fiber intake can lead to constipation, which is a risk factor.
Heavy lifting: Straining while lifting heavy objects can contribute to the development of hemorrhoids.
Chronic cough or sneezing: Persistent, forceful coughing or sneezing can increase abdominal pressure.
When does a haemorrhoid become painful?
Hemorrhoids become painful when there is inflammation or swelling in the blood vessels in the rectal or anal area. This can occur due to various factors, including:
Thrombosis: When a blood clot forms within a hemorrhoidal vein, causing significant pain and swelling.
Strangulation: If internal hemorrhoids prolapse (extend outside the anal opening) and the blood supply is cut off, it can lead to pain.
Inflammation: Irritation and inflammation of hemorrhoids, often due to straining during bowel movements or other contributing factors.
External hemorrhoids: These can be more painful than internal ones, as they are located under the skin around the anus and are more sensitive.
What are the complications of haemorrhoidectomy
Pain and Discomfort: Postoperative pain is common, and patients may experience discomfort during the recovery period.
Bleeding: Some bleeding is normal after surgery, but excessive bleeding may occur in rare cases.
Infection: Infections at the surgical site are possible, though they are uncommon.
Urinary Retention: Difficulty in passing urine may occur temporarily after the procedure.
Anal Stenosis: Narrowing of the anal opening, though rare, can occur as a result of scarring.
Fecal Incontinence: Loss of control over bowel movements is a rare but potential complication.
Delayed Healing: In some cases, the surgical site may take longer to heal than expected.
Recurrence of Hemorrhoids: While hemorrhoidectomy is effective, there is a small chance that hemorrhoids may return.
Allergic Reactions: Rarely, individuals may experience allergic reactions to medications or materials used during surgery.
What are the complications of haemorrhoids?
Thrombosis: Formation of blood clots in hemorrhoidal veins, leading to pain and swelling.
Bleeding: Hemorrhoids can cause bleeding, especially during bowel movements.
Prolapse: Internal hemorrhoids may protrude outside the anal opening, causing discomfort.
Strangulation: Prolapsed hemorrhoids may have blood supply issues, resulting in pain.
Infection: Scratching or irritation can lead to infections in the anal area.
Anaemia: Chronic bleeding from hemorrhoids may contribute to low blood iron levels and anemia.
Anal Fissures: Tears in the anal lining can occur in conjunction with hemorrhoids, causing pain.
-
Gastro-Oesophageal Reflux Disease
Doctor Instruction:
You are a Foundation Year 1 Doctor working in the Emergency Department. Your next patient is a 42-year-old woman (Anne) presenting with abdominal pain. Please take a history and perform an appropriate examination.
Patient History:
Anne, a 42-year-old retired hairdresser.
This morning at around 3am, you woke up from having tummy pain. Described as a sharp/burning sensation that started at the bottom chest centrally and radiated up to the neck. It is intermittent and lasts for a few seconds. Pain score: 5/10. You are known to have angina, and so you took a GTN spray, but it didn't help. You feel a bit nauseous but no vomiting; you had some retching (and a bad taste in the back of the throat). Pain tends to be worsened or triggered when you try to go back to bed and lay flat.
If asked specifically, you remember having quite a big family meal when your friend came to visit the night before.
No weight loss. No tiredness. No erosion in teeth. No bad-smelling mouth. No lump in the throat. No bloating. No nocturnal cough. No hoarse voice. Bowels working normally with no bloody stool. No breathing difficulty. No dysphagia. No LOC. No dizziness. No palpitation. No obvious chest pain.
Ideas, Concerns, Expectations:
You are not sure what is going on. You are worried that you had a heart attack and may die because of this since it is quite close to the chest. You want to be seen by a cardiologist and have some medications to help prevent having this pain again. You want to live!
Past Medical History:
Hypertension
Stable angina - well-controlled
Obesity
Chronic Lower Back Pain
Drug History:
Amlodipine, GTN spray PRN, Atovastatin, ibuprofen
NKDA
Family History:
Type 2 DM (Dad, age 44)
Colon Cancer (Dad, age 65)
Social History:
Smoker – 10 cigarettes/day for 20 + years
Drink a small glass of gin and tonic every night
Hairdresser
Drink 2 cups of coffee a day.
Examination Findings:
The patient is alert + comfortable at rest, with no signs of breathing difficulties.
No clinical signs of anaemia.
Some mild discomfort palpating the epigastric region.
Abdominal examination is otherwise normal.
PR exam is normal - no melena or blood in the stool.
Differentials:
GORD
Gastritis
Peptic ulcer
Hiatus Hernia
Oesophagitis / Oesophageal spasm
To rule out cardiovascular causes: Stable Angina / ACS / AAA
Investigations:
Bedside:
Observations
ECG – rule out cardiac cause
Bloods:
FBC, CRP, U&Es, LFTs, Bone Profile, Troponin (if suspecting cardiac cause)
Imaging:
CXR/AXR (?Hiatus hernia)
Special Tests:
Consider serology/ urea breath test/ stool antigen, rapid urease test (H-pylori testing - ensure not taken PPI 2 weeks prior to testing)
Barium swallow - assess dynamics, assess motility disorder, assess for hiatus hernia
Oesophageal pH monitoring / Manometry - Assess for motility & regurgitative Disorders
Consider OGD (Savary-Miller grading/ Los Angeles Classification) - allows direct visualisation and biopsy for histology.
Data Interpretation:
Patient Details: Alexander Great
Age: 42
Date of Request: 18/04/2023
Value
Reference Range
Hb
125 g/L
115 - 165 g/L
White Cell Count
7.5 x10^9/L
3.6 - 11.0 x10^9/L
Platelets
257 x10^9/L
140 - 400 x10^9/L
Haematocrit
0.47 x10^12/L
0.40 - 0.54 x10^12/L
MCV
94 fL
80 - 100 fL
Neutrophils
3.7 x10^9/L
1 - 7.5 x10^9/L
Monocytes
0.7 x10^9/L
0.2 - 0.8 x10^9/L
Lymphocytes
3 x10^9/L
1 - 4 x10^9/L
Basophils
0.03 x10^9/L
0.02 - 0.1
Eosinophils
0.1
0.1 - 0.4
H. Pylori Stool Antigen Test
Negative
Interpretation of Blood Results:
ree
Interpretation of OGD Image:
Management (GORD):
Conservative:
Lifestyle changes: stop smoking, weight loss, reduce alcohol intake, sleep more upright, small + regular meals, avoid eating big meals/ alcohol/ hot drinks before bed, avoid triggering diet e.g. spicy food, citrus, chocolate, caffeine, carbonated drinks, alcohol, manage stress level
Review medications that can cause reflux, e.g. NSAID, steroids, bisphosphonates, nitrates, calcium channel blockers, alpha/beta agonists, theophylline, anticholinergics
Antacids e.g. Gaviscon
PPI e.g. omeprazole
H2 antagonist e.g. Ranitidine
Patient Education
Safety netting for uncontrolled and red flag symptoms e.g. ACS
Medical:
Eradication therapy if tested positive for H. Pylori (PPI plus 2 antibiotics e.g. amoxicillin and clarithromycin) for 7 days.
Surgical:
Surgery for reflux e.g. fundoplication, magnetic sphincter augmentation.
Viva questions:
What are the complications of untreated acid reflux?
Esophagitis: Inflammation and pain in the esophagus.
Barrett's Esophagus: Increased risk of esophageal cancer.
Strictures: Narrowing of the esophagus.
Esophageal Ulcers: Painful sores in the esophagus.
Respiratory Issues: Coughing, wheezing, and asthma exacerbation.
Dental Problems: Tooth enamel erosion and oral health issues.
Chronic Cough: Persistent cough unrelated to respiratory problems.
Laryngitis/Voice Changes: Hoarseness and vocal cord inflammation.
Asthma Aggravation: Worsening of asthma symptoms.
Difficulty Swallowing: Dysphagia due to esophageal changes.
Esophageal Cancer: Increased cancer risk over time.
What are the complications of long-term management with omeprazole?
Electrolyte disturbance e.g. magnesium
Low bone mineral density - interference in gastric pH which can alter calcium absorption
What is Barrett's Oesophagus?
Barrett's esophagus develops due to chronic acid reflux (GERD). Acid irritates the esophagus, prompting the lining to transform into a type more resistant to acid, called columnar cells. This change is known as metaplasia, resulting in Barrett's epithelium. This condition increases the risk of esophageal cancer, making regular monitoring crucial.
What are the red flag symptoms or signs for urgent OGD?
Haematemesis or melena
Dysphagia
Unintentional weight loss
Treatment-resistant
Early satiety
Recurrent vomitting