Meningioma
-
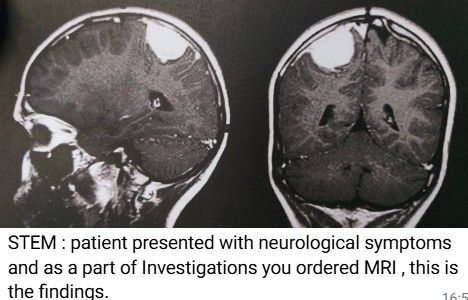
- Identify hyperdense mass
Answer: Meningioma
Usually extra-axial, well-circumscribed, often hyperdense on CT.- Where does it arise from
Answer: Arachnoid cap cells
Correct. These are in the arachnoid villi of the meninges.- What structure might it compress
Answer: Superior sagittal sinus
True for parasagittal meningiomas.
Can also compress adjacent cortex → neurological deficits.- What structures does it lie between
Answer: Falx and cerebral hemisphere
Correct. Extra-axial, attached to dura of falx.- What will patient present with
Answer: Monoparesis contralateral lower limb
This is classic for parasagittal lesion affecting the leg area of primary motor cortex.- What area of brain affected
Answer: Motor area 4
Brodmann area 4 = primary motor cortex.
Can also mention paracentral lobule specifically for leg involvement.- What area body represented medial side of motor area
Answer: Lower Limb
Lateral = face and hand; medial = leg and foot.- Which layer of meninges is the meningioma attached to?
Answer: Dura mater
Meningiomas are dural-based tumours, hence the “dural tail” sign on imaging.- What is major vein draining brain parenchyma
Answer: Internal cerebral veins / deep cerebral veins
Superficial drainage → superficial cortical veins → dural sinuses.- What drains into dural sinuses
Answer: Cerebral veins (superficial and deep), diploic veins, emissary veins, CSF via arachnoid granulations
- Branches of middle cerebral artery
Lateral lenticulostriate arteries (deep)
Cortical branches → frontal, parietal, temporal, insular cortices- Signs of MCA infarction
Contralateral hemiplegia and hemianesthesia (face and upper limb > leg)
Contralateral homonymous hemianopia
Aphasia if left hemisphere dominant
Neglect if right hemisphere -
Typical exam stem:
A 55-year-old woman presents with gradually progressive weakness of one leg. She also reports focal seizures affecting the same limb. Examination shows monoparesis of the contralateral lower limb with increased tone and brisk reflexes.
Most likely diagnosis:
A Parasagittal meningiomaThe tumour grows along the Falx cerebri and compresses the medial surface of the brain where the leg motor area lies in the Paracentral lobule of the Primary motor cortex.
Because the Corticospinal tract crosses in the Pyramidal decussation, the weakness appears on the opposite side.
Classic MRCS clinical features
Feature Reason
Contralateral lower limb monoparesis Leg area of motor cortex compressed
Focal motor seizures in the leg Cortical irritation
Slow progression Typical for benign meningioma
Upper motor neuron signs (hyperreflexia, Babinski) Corticospinal tract involvement
Imaging clueMRI usually shows an extra-axial tumour with a dural attachment (“dural tail”), typical of a Meningioma.
“Falx tumour → opposite leg weak.”
Falx / parasagittal location
Leg motor cortex affected
Weakness contralateral -
- Parasagittal meningioma
Tumour: Parasagittal meningioma
Typical presentation
Gradually progressive contralateral lower limb weakness
Focal seizures in the leg
UMN signs
Why
Compression of the Paracentral lobule (leg area of the Primary motor cortex).Exam clue
Progressive leg weakness + seizures → parasagittal meningioma.
- Acoustic neuroma (vestibular schwannoma)
Tumour: Vestibular schwannoma
Typical presentation
Unilateral hearing loss
Tinnitus
Balance problems
Later:
Facial numbness
Facial weakness
Why
Compression of:Vestibulocochlear nerve (CN VIII)
Facial nerve (CN VII)
Exam clue
Progressive unilateral deafness.
- Pituitary adenoma
Tumour: Pituitary adenoma
Typical presentation
Bitemporal hemianopia
Why
Compression of the Optic chiasm.Other clues:
Hormonal symptoms (galactorrhoea, acromegaly, Cushing's).
Exam clue
Loss of temporal visual fields.
- Cerebellopontine angle tumour
Often a Vestibular schwannoma.
Symptoms
Hearing loss
Facial numbness
Ataxia
Structures involved:
Trigeminal nerve
Facial nerve
Vestibulocochlear nerve
Exam clue
Multiple cranial nerve deficits in the cerebellopontine angle.
- Frontal lobe tumour
Commonly a Glioma.
Typical presentation
Personality change
Disinhibition
Poor judgement
Sometimes urinary incontinence
Structure affected:
Frontal lobe
Exam clue
Behavioural change before neurological deficit.
✅ Very high-yield MRCS pattern
Symptom Likely tumour
Leg weakness Parasagittal meningioma
Unilateral deafness Vestibular schwannoma
Bitemporal hemianopia Pituitary adenoma
Behaviour change Frontal lobe tumour
Multiple cranial nerve palsies CPA tumour
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login